

KIT mutation analysis in mast cell neoplasms: recommendations of the European Competence Network on Mastocytosis
- PMID: 25650093
- PMCID: PMC4522520
- DOI: 10.1038/leu.2015.24
KIT mutation analysis in mast cell neoplasms: recommendations of the European Competence Network on Mastocytosis
Abstract
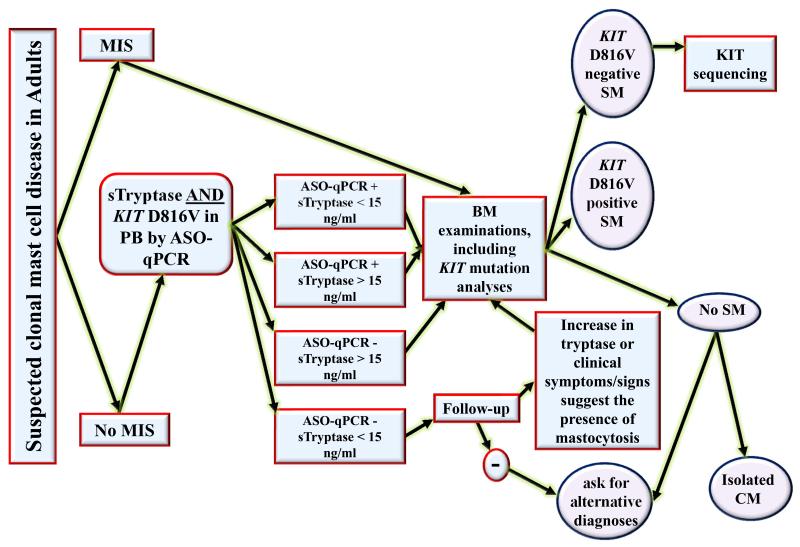
Although acquired mutations in KIT are commonly detected in various categories of mastocytosis, the methodologies applied to detect and quantify the mutant type and allele burden in various cells and tissues are poorly defined. We here propose a consensus on methodologies used to detect KIT mutations in patients with mastocytosis at diagnosis and during follow-up with sufficient precision and sensitivity in daily practice. In addition, we provide recommendations for sampling and storage of diagnostic material as well as a robust diagnostic algorithm. Using highly sensitive assays, KIT D816V can be detected in peripheral blood leukocytes from most patients with systemic mastocytosis (SM) that is a major step forward in screening and SM diagnosis. In addition, the KIT D816V allele burden can be followed quantitatively during the natural course or during therapy. Our recommendations should greatly facilitate diagnostic and follow-up investigations in SM in daily practice as well as in clinical trials. In addition, the new tools and algorithms proposed should lead to a more effective screen, early diagnosis of SM and help to avoid unnecessary referrals.
Figures
References
-
- Krishnaswamy G, Ajitawi O, Chi DS. The human mast cell: an overview. Methods Mol Biol. 2006;315:13–34. - PubMed
-
- Miettinen M, Lasota J. KIT (CD117): a review on expression in normal and neoplastic tissues, and mutations and their clinicopathologic correlation. Appl Immunohistochem Mol Morphol. 2005;13:205–220. - PubMed
-
- Ashman LK, Ferrao P, Cole SR, Cambareri AC. Effects of mutant c-kit in early myeloid cells. Leuk Lymphoma. 2000;37:233–243. - PubMed
-
- Kirshenbaum AS, Goff JP, Semere T, Foster B, Scott LM, Metcalfe DD. Demonstration that human mast cells arise from a progenitor cell population that is CD34(+), c-kit(+), and expresses aminopeptidase N (CD13) Blood. 1999;94:2333–2342. - PubMed
-
- Matarraz S, Lopez A, Barrena S, Fernandez C, Jensen E, Flores J, et al. The immunophenotype of different immature, myeloid and B-cell lineage-committed CD34+ hematopoietic cells allows discrimination between normal/reactive and myelodysplastic syndrome precursors. Leukemia. 2008;22:1175–1183. - PubMed
