

Whole-genome and multisector exome sequencing of primary and post-treatment glioblastoma reveals patterns of tumor evolution
- PMID: 25650244
- PMCID: PMC4352879
- DOI: 10.1101/gr.180612.114
Whole-genome and multisector exome sequencing of primary and post-treatment glioblastoma reveals patterns of tumor evolution
Abstract
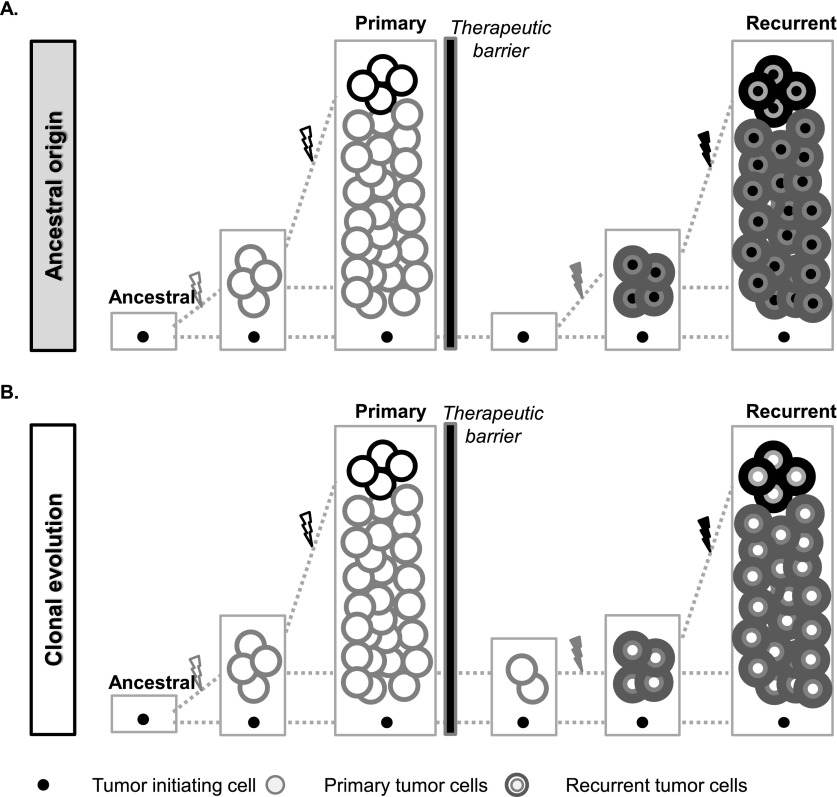
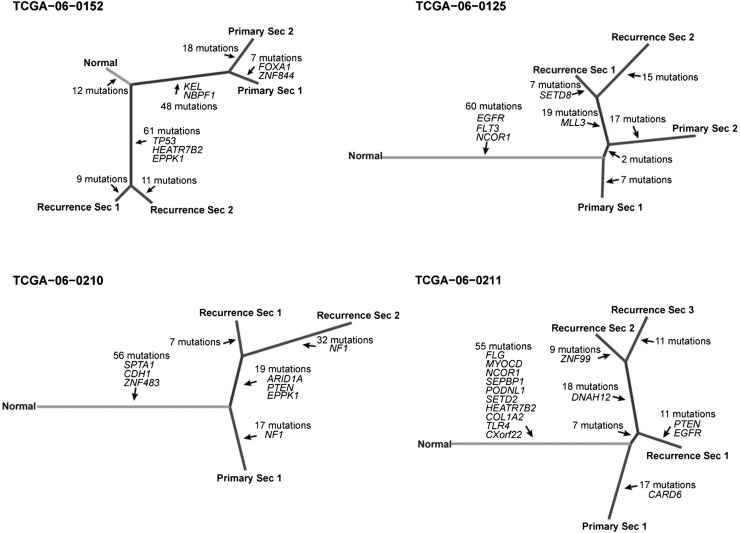
Glioblastoma (GBM) is a prototypical heterogeneous brain tumor refractory to conventional therapy. A small residual population of cells escapes surgery and chemoradiation, resulting in a typically fatal tumor recurrence ∼ 7 mo after diagnosis. Understanding the molecular architecture of this residual population is critical for the development of successful therapies. We used whole-genome sequencing and whole-exome sequencing of multiple sectors from primary and paired recurrent GBM tumors to reconstruct the genomic profile of residual, therapy resistant tumor initiating cells. We found that genetic alteration of the p53 pathway is a primary molecular event predictive of a high number of subclonal mutations in glioblastoma. The genomic road leading to recurrence is highly idiosyncratic but can be broadly classified into linear recurrences that share extensive genetic similarity with the primary tumor and can be directly traced to one of its specific sectors, and divergent recurrences that share few genetic alterations with the primary tumor and originate from cells that branched off early during tumorigenesis. Our study provides mechanistic insights into how genetic alterations in primary tumors impact the ensuing evolution of tumor cells and the emergence of subclonal heterogeneity.
© 2015 Kim et al.; Published by Cold Spring Harbor Laboratory Press.
Figures
References
-
- Aparicio S, Caldas C. 2013. The implications of clonal genome evolution for cancer medicine. N Engl J Med 368: 842–851. - PubMed
-
- Bao S, Wu Q, McLendon RE, Hao Y, Shi Q, Hjelmeland AB, Dewhirst MW, Bigner DD, Rich JN. 2006. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 444: 756–760. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 CA083639-12/CA/NCI NIH HHS/United States
- R01 CA188228/CA/NCI NIH HHS/United States
- R01 CA086335/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- U24 CA143882/CA/NCI NIH HHS/United States
- HHSN261201000057C/CA/NCI NIH HHS/United States
- R01 CA190121/CA/NCI NIH HHS/United States
- R25 CA094186/CA/NCI NIH HHS/United States
- CA143883/CA/NCI NIH HHS/United States
- CA016672/CA/NCI NIH HHS/United States
- HHSN261201000057I/CA/NCI NIH HHS/United States
- P30 CA138292/CA/NCI NIH HHS/United States
- HHSN261201000057C/PHS HHS/United States
- P50 CA083639/CA/NCI NIH HHS/United States
- U24 CA143883/CA/NCI NIH HHS/United States
- R01 CA163722/CA/NCI NIH HHS/United States
- P50 CA127001/CA/NCI NIH HHS/United States
- P01 CA085878/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous