

Hemorrhagic complications in pediatric cardiac patients on extracorporeal membrane oxygenation: an analysis of the Extracorporeal Life Support Organization Registry
- PMID: 25651048
- PMCID: PMC4668708
- DOI: 10.1097/PCC.0000000000000345
Hemorrhagic complications in pediatric cardiac patients on extracorporeal membrane oxygenation: an analysis of the Extracorporeal Life Support Organization Registry
Abstract
Objectives: To determine the prevalence of and risk factors for hemorrhagic complications in children with cardiac disease requiring extracorporeal membrane oxygenation.
Design: Retrospective review of the Extracorporeal Life Support Organization Registry (2002-2013).
Setting: Participating Extracorporeal Life Support Organization centers.
Patients: Patients less than 18 years old on extracorporeal membrane oxygenation.
Interventions: None.
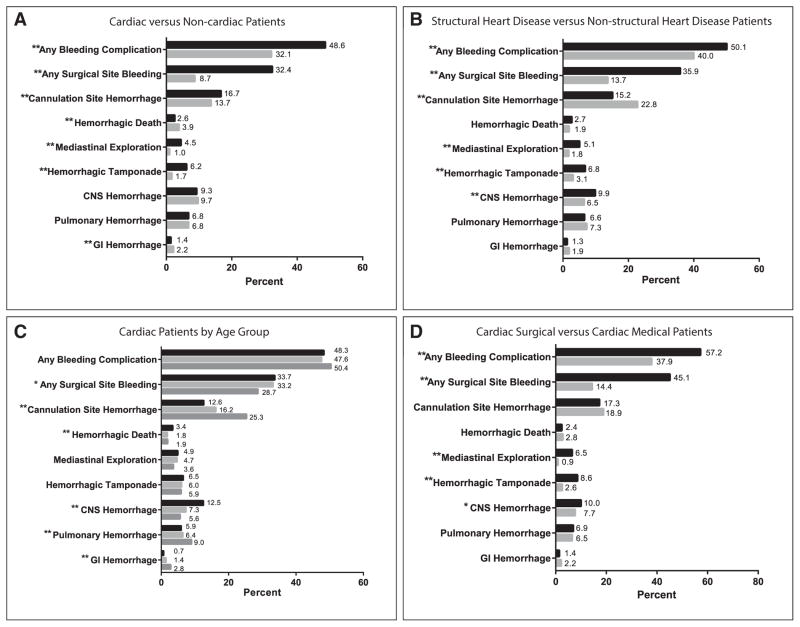
Measurements and main results: Of 21,845 patients requiring extracorporeal membrane oxygenation during the study period, 8,905 (41%) had cardiac disease, and 79% of whom (6,995) had cardiac surgery. Hemorrhagic complications occurred in 8,480 patients (39% of overall cohort), with higher rates in cardiac versus noncardiac patients (49% vs 32%; p < 0.0001) related to cannulation and surgical site bleeding. Cardiac surgical patients had higher rates of hemorrhage compared with cardiac medical patients (57% vs 38%; p < 0.0001), and cardiac patients with hemorrhage had higher extracorporeal membrane oxygenation mortality compared with those without (42% vs 22% in medical patients and 34% vs 20% in surgical patients; both p < 0.0001). In multivariable analysis in both the cardiac medical and surgical groups, hemorrhage risk was higher in children greater than 1 year old and in patients with longer extracorporeal membrane oxygenation duration. Additional independent risk factors for hemorrhage in cardiac surgical patients included pre-extracorporeal membrane oxygenation mediastinal exploration (odds ratio, 3.6; 95% CI, 2.1-6.3), Society of Thoracic Surgeons morbidity category 4-5 (odds ratio, 1.2; 95% CI, 1.03-1.5), cannulation less than 24 hours after surgery (odds ratio, 1.6; 95% CI, 1.3-1.9), and longer cardiopulmonary bypass time (≥ 282 min [upper quartile]; odds ratio, 1.5; 95% CI, 1.3-1.9).
Conclusions: In this large, multicenter analysis, hemorrhagic complications occurred in nearly half of children with heart disease on extracorporeal membrane oxygenation and were associated with a significant mortality risk. Several factors were associated with hemorrhagic complications in cardiac surgical patients including pre-extracorporeal membrane oxygenation mediastinal exploration, greater surgical complexity, early postoperative cannulation, and longer bypass times. Whether these risks can be mitigated by modifying or delaying systemic anticoagulation requires further investigation.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Muntean W. Coagulation and anticoagulation in extracorporeal membrane oxygenation. Artif Organs. 1999;23:979–983. - PubMed
-
- Oliver WC. Anticoagulation and coagulation management for ECMO. Semin Cardiothorac Vasc Anesth. 2009;13:154–175. - PubMed
-
- Gaffney AM, Wildhirt SM, Griffin MJ, et al. Extracorporeal life support. BMJ. 2010;341:982–986. - PubMed
-
- Suzuki Y, Yamauchi S, Daitoku K, et al. Extracorporeal membrane oxygenation circulatory support after congenital cardiac surgery. ASAIO J. 2009;55:53–57. - PubMed
-
- Haines NM, Rycus PT, Zwischenberger JB, et al. Extracorporeal Life Support Registry Report 2008: Neonatal and pediatric cardiac cases. ASAIO J. 2009;55:111–116. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
