

Review
doi: 10.1016/j.cmet.2015.01.013.
The genetic landscape of cardiomyopathy and its role in heart failure
Affiliations
- PMID: 25651172
- PMCID: PMC4331062
- DOI: 10.1016/j.cmet.2015.01.013
Item in Clipboard
Review
The genetic landscape of cardiomyopathy and its role in heart failure
Cell Metab.
.
Abstract
Heart failure is highly influenced by heritability, and nearly 100 genes link to familial cardiomyopathy. Despite the marked genetic diversity that underlies these complex cardiovascular phenotypes, several key genes and pathways have emerged. Hypertrophic cardiomyopathy is characterized by increased contractility and a greater energetic cost of cardiac output. Dilated cardiomyopathy is often triggered by mutations that disrupt the giant protein titin. The energetic consequences of these mutations offer molecular targets and opportunities for new drug development and gene correction therapies.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
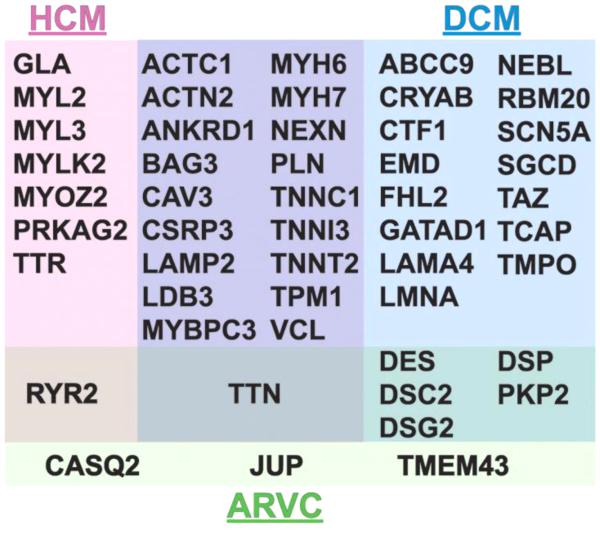
Shown are the genes that have been linked to human inherited cardiomyopathy. Those genes responsible for HCM (pink) and DCM (blue). There are a number of genes that cause both HCM and DCM (purple). Mutations in genes encoding desmosomal and other proteins cause Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC, green) and there is overlap between mutations in these genes that lead to other forms of cardiomyopathy.
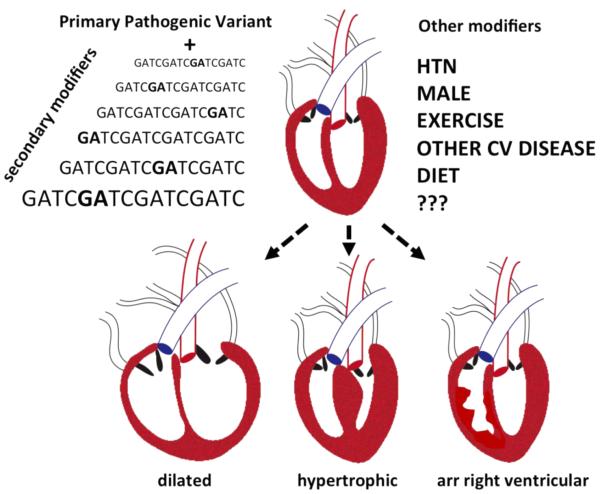
Familial studies for inherited cardiomyopathy often demonstrate a primary pathogenic variant, and pathogenic variants differ in their effect on phenotypic outcome. Each genome contains many additional variants that serve to modify the expression of the primary pathogenic variant. These secondary modifers may be common or rare in the population. In addition to these genetic modifiers, comorbidities, environmental factors, and sex modulate the expression of cardiomyopathy. The manifestation of cardiomyopathy varies over the lifetime of the individual. Those mutations, or combinations of mutations, with the most potent effect on phenotype manifest earlier in life. Milder mutations may not express until later in life or may remain subclinical throughout the lifetime of the individual. (Dilated, DCM; hypertrophic HCM; arr right ventricular, ARVC).
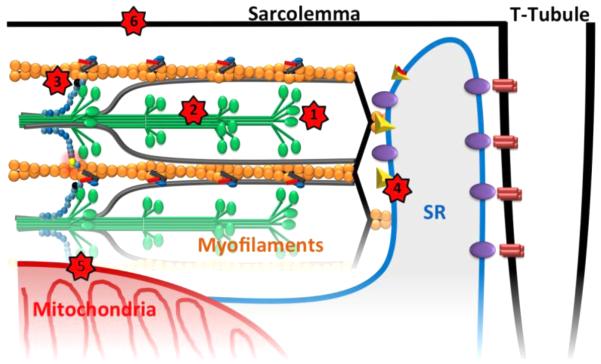
Myosin heads protrude from the thick filaments (green) to interact with actin containing thin filaments (yellow). Multiple sites throughout the sarcomere and cardiomyocyte are now the targets for new drug development for heart failure (Red stars). 1. Small molecules like omecamtiv are aimed at myosin ATPase activity to increase or decrease contractility. 2. Antisense or RNAi approaches are being tested to silence mutant alleles but not normal alleles. 3. cMyBP-C phosphorylation can be modified through kinase/phosphatases to modulate its “brake effect” on cross-bridge cycling. 4. Calcium handing in the sarcoplasmic reticulum is a target in development. 5. Palmitoyltransferase-1 can be altered using perhexiline to shift metabolic substrate usage from fatty acid oxidation to glycolysis. 6. The regulation of nitric oxide synthase can be used to change cellular redox state and prevent glutathionylation and dysregulation of myofilament proteins.
References
-
- Alpert NR, Mohiddin SA, Tripodi D, Jacobson-Hatzell J, Vaughn-Whitley K, Brosseau C, Warshaw DM, Fananapazir L. Molecular and phenotypic effects of heterozygous, homozygous, and compound heterozygote myosin heavy-chain mutations. American journal of physiology. Heart and circulatory physiology. 2005;288:H1097–1102. - PubMed
-
- Arad M, Seidman JG, Seidman CE. Phenotypic diversity in hypertrophic cardiomyopathy. Hum Mol Genet. 2002;11:2499–2506. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
