

Tenofovir-based preexposure prophylaxis for HIV infection among African women
- PMID: 25651245
- PMCID: PMC4341965
- DOI: 10.1056/NEJMoa1402269
Tenofovir-based preexposure prophylaxis for HIV infection among African women
Abstract
Background: Reproductive-age women need effective interventions to prevent the acquisition of human immunodeficiency virus type 1 (HIV-1) infection.
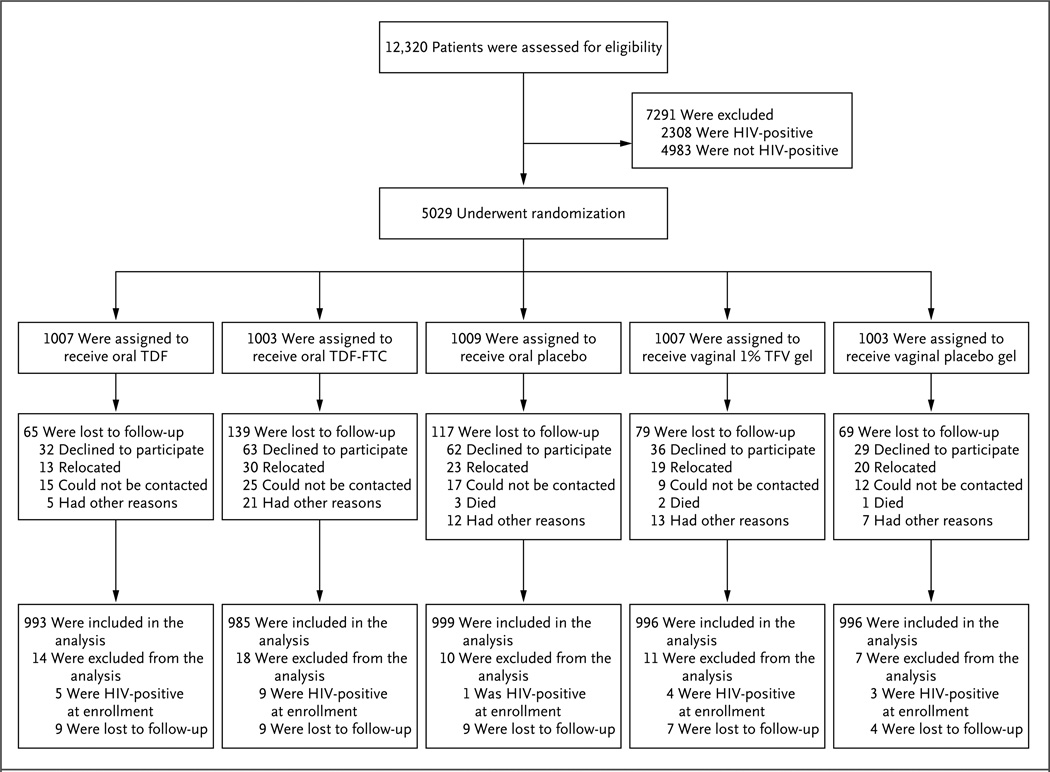
Methods: We conducted a randomized, placebo-controlled trial to assess daily treatment with oral tenofovir disoproxil fumarate (TDF), oral tenofovir-emtricitabine (TDF-FTC), or 1% tenofovir (TFV) vaginal gel as preexposure prophylaxis against HIV-1 infection in women in South Africa, Uganda, and Zimbabwe. HIV-1 testing was performed monthly, and plasma TFV levels were assessed quarterly.
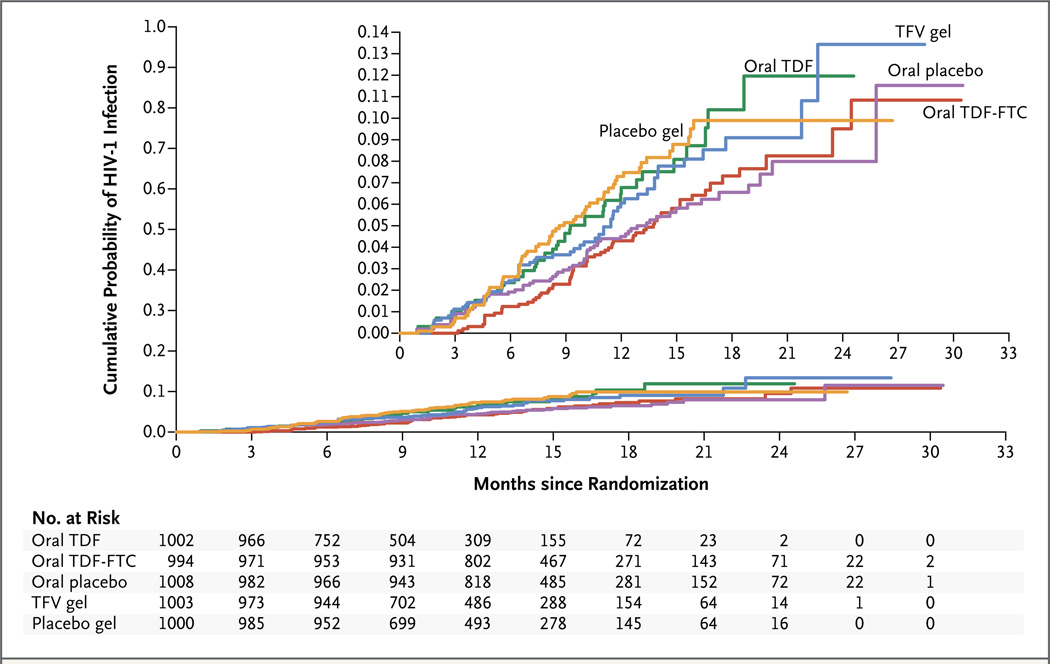
Results: Of 12,320 women who were screened, 5029 were enrolled in the study. The rate of retention in the study was 91% during 5509 person-years of follow-up. A total of 312 HIV-1 infections occurred; the incidence of HIV-1 infection was 5.7 per 100 person-years. In the modified intention-to-treat analysis, the effectiveness was -49.0% with TDF (hazard ratio for infection, 1.49; 95% confidence interval [CI], 0.97 to 2.29), -4.4% with TDF-FTC (hazard ratio, 1.04; 95% CI, 0.73 to 1.49), and 14.5% with TFV gel (hazard ratio, 0.85; 95% CI, 0.61 to 1.21). In a random sample, TFV was detected in 30%, 29%, and 25% of available plasma samples from participants randomly assigned to receive TDF, TDF-FTC, and TFV gel, respectively. Independent predictors of TFV detection included being married, being older than 25 years of age, and being multiparous. Detection of TFV in plasma was negatively associated with characteristics predictive of HIV-1 acquisition. Elevations of serum creatinine levels were seen more frequently among participants randomly assigned to receive oral TDF-FTC than among those assigned to receive oral placebo (1.3% vs. 0.2%, P=0.004). We observed no significant differences in the frequencies of other adverse events.
Conclusions: None of the drug regimens we evaluated reduced the rates of HIV-1 acquisition in an intention-to-treat analysis. Adherence to study drugs was low. (Funded by the National Institutes of Health; VOICE ClinicalTrials.gov number, NCT00705679.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Preventing HIV in women--still trying to find their VOICE.N Engl J Med. 2015 Feb 5;372(6):564-6. doi: 10.1056/NEJMe1415750. N Engl J Med. 2015. PMID: 25651251 No abstract available.
-
Pre-exposure prophylaxis in women fails to prevent HIV infection in African study.BMJ. 2015 Feb 6;350:h717. doi: 10.1136/bmj.h717. BMJ. 2015. PMID: 25663035 No abstract available.
-
Preexposure prophylaxis for HIV infection.N Engl J Med. 2015 Apr 30;372(18):1767-8. doi: 10.1056/NEJMc1502749. N Engl J Med. 2015. PMID: 25923561 No abstract available.
-
VOICE reveals the need to improve adherence in PrEP trials.AIDS. 2015 Jul 31;29(12):N9. doi: 10.1097/QAD.0000000000000693. AIDS. 2015. PMID: 26244400 No abstract available.
-
Pre-exposure prophylaxis for the prevention of HIV infection: a new prevention paradigm?Farm Hosp. 2016 May 1;40(3):219-24. doi: 10.7399/fh.2016.40.3.10439. Farm Hosp. 2016. PMID: 27145390 English.
References
-
- Thigpen MC, Kebaabetswe PM, Paxton LA, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med. 2012;367:423–434. - PubMed
-
- Choopanya K, Martin M, Suntharasamai P, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2013;381:2083–2090. - PubMed
-
- Centers for Disease Control and Prevention. Preexposure prophylaxis for the prevention of HIV infection in the United States — 2014. U.S. Public Health Service. 2014 ( http://www.cdc.gov/hiv/pdf/prepprovidersupplement2014.pdf)
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical