

Mechanisms of airway hyper-responsiveness in asthma: the past, present and yet to come
- PMID: 25651937
- PMCID: PMC4386586
- DOI: 10.1111/cea.12506
Mechanisms of airway hyper-responsiveness in asthma: the past, present and yet to come
Abstract
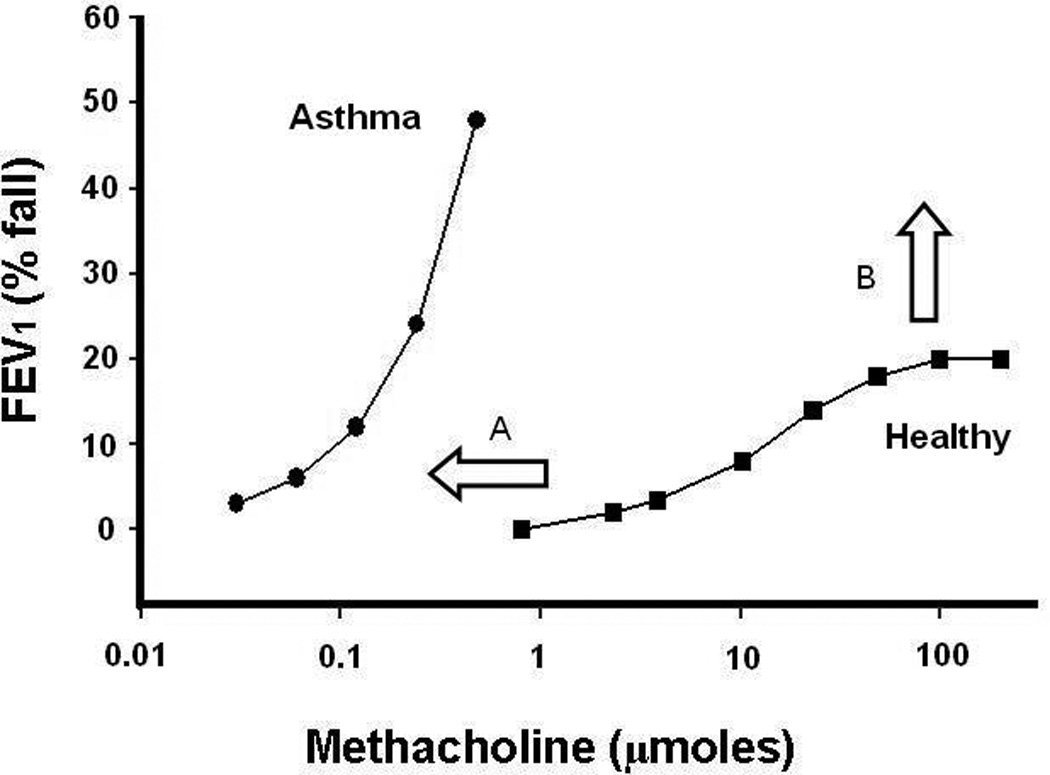
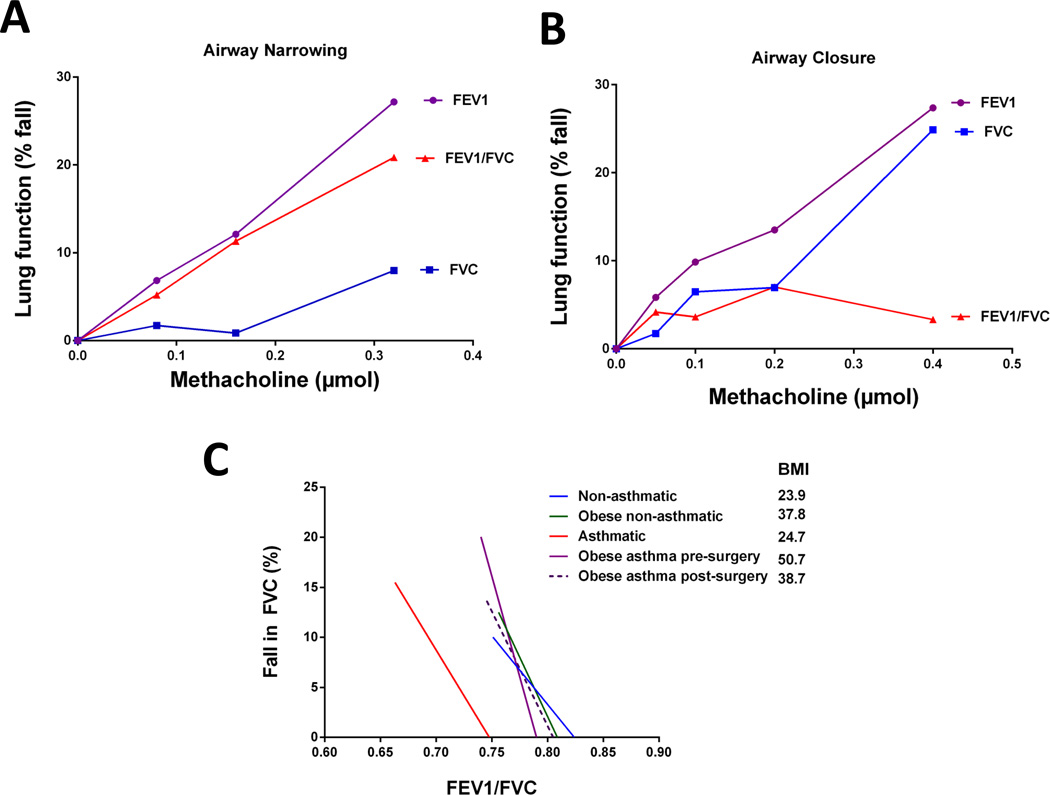
Airway hyper-responsiveness (AHR) has long been considered a cardinal feature of asthma. The development of the measurement of AHR 40 years ago initiated many important contributions to our understanding of asthma and other airway diseases. However, our understanding of AHR in asthma remains complicated by the multitude of potential underlying mechanisms which in reality are likely to have different contributions amongst individual patients. Therefore, the present review will discuss the current state of understanding of the major mechanisms proposed to contribute to AHR and highlight the way in which AHR testing is beginning to highlight distinct abnormalities associated with clinically relevant patient populations. In doing so we aim to provide a foundation by which future research can begin to ascribe certain mechanisms to specific patterns of bronchoconstriction and subsequently match phenotypes of bronchoconstriction with clinical phenotypes. We believe that this approach is not only within our grasp but will lead to improved mechanistic understanding of asthma phenotypes and we hoped to better inform the development of phenotype-targeted therapy.
© 2015 John Wiley & Sons Ltd.
Figures
References
-
- Cockcroft DW, Killian DN, Mellon JJ, Hargreave FE. Bronchial reactivity to inhaled histamine: a method and clinical survey. Clin Allergy. 1977;7(3):235–243. - PubMed
-
- Tiffeneau R, Beauvallet M. Epreuve de bronchoconstriction et de bronchodilation par aerosols. Bull Acad Med. 1945;129:165–168.
-
- de Vries, Tammeling GJ, Orie NG. [Hyperreactivity of the bronchi in bronchial asthma and chronic bronchitis] Ned Tijdschr Geneeskd. 1962;106:2295–2296. - PubMed
-
- Parker CD, Bilbo RE, Reed CE. METHACHOLINE AEROSOL AS TEST FOR BRONCHIAL ASTHMA. Arch Intern Med. 1965;115:452–458. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
