

Nebulized magnesium for moderate and severe pediatric asthma: A randomized trial
- PMID: 25652104
- PMCID: PMC7167999
- DOI: 10.1002/ppul.23158
Nebulized magnesium for moderate and severe pediatric asthma: A randomized trial
Abstract
Background: Intravenous magnesium sulfate, a rescue therapy added to bronchodilator and systemic steroid therapy for moderate and severe asthma, is uncommonly administered. We hypothesized that nebulized magnesium would confer benefit without undue risk.
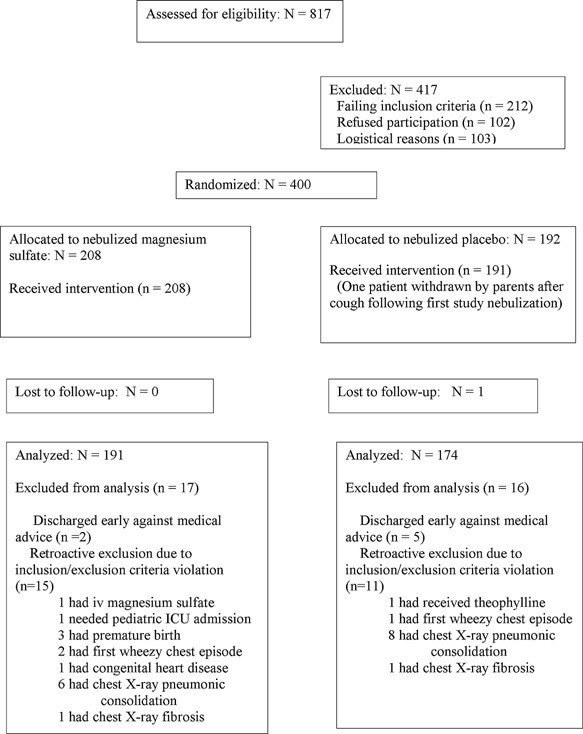
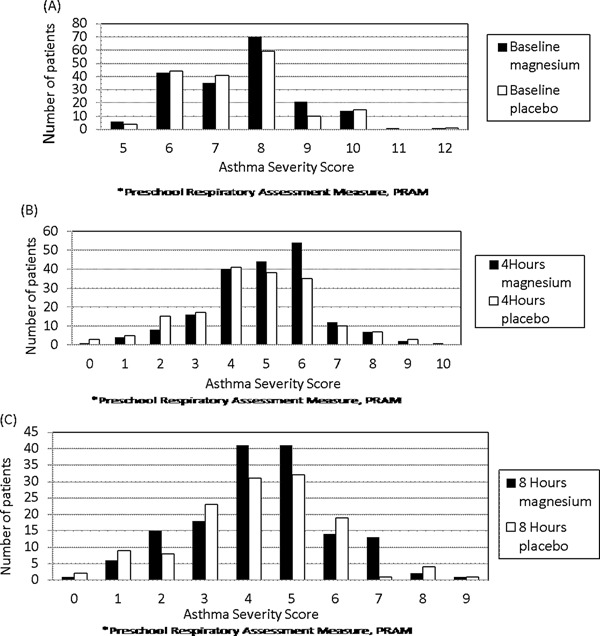
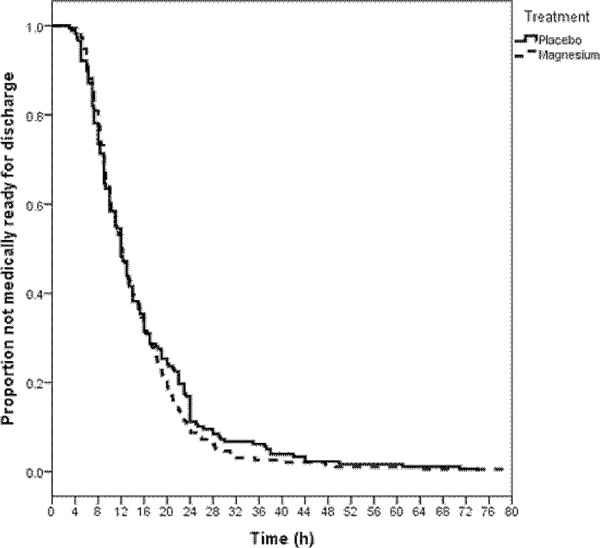
Design and methods: Patients aged 2 to 14 y with moderate and severe asthma (PRAM severity score ≥ 4) admitted to infirmary/observation unit care were randomized double-blind on admission to receive 800 mg nebulized magnesium or normal saline placebo after all received intensive therapy with combined nebulized albuterol-ipratropium and intravenous methylprednisolone. Time to medical readiness for discharge was the primary outcome; sample size was chosen to detect a 15% absolute improvement. Improvement over time in PRAM severity score and other secondary outcomes were compared for the overall group and severe asthma subset.
Results: One hundred and ninety-one magnesium sulfates and 174 placebo patients met criteria for analysis. The groups were similar with mean baseline PRAM scores >7. Blinded active therapy significantly increased blood magnesium level 2 hr post-treatment completion compared to placebo, 0.85 vs 0.82 mmol/L, P = 0.001. There were no important adverse effects. Accelerated failure time analysis showed a non-significantly shortened time to medical readiness for discharge of 14% favoring the magnesium sulfate group, OR = 1.14, 95% CI 0.93 to 1.40, P = 0.20. Mean times until readiness for discharge were 14.7 hr [SD 9.7] versus 15.6 hr [SD 11.3] for the investigational and placebo groups, respectively, P = 0.41.
Conclusions: Adding nebulized magnesium to combined nebulized bronchodilator and systemic steroid therapy failed to significantly shorten time to discharge of pediatric patients with moderate or severe asthma.
Trial registration: ClinicalTrials.gov NCT01584726.
Keywords: bronchodilator; nebulization; pediatric emergency.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Powell C, Dwan K, Milan SJ, Beasley R, Hughes R, Knopp‐Sihota JA, Rowe BH. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev 2012; 12:CD003898. - PubMed
-
- British Thoracic Society and Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A national clinical guideline. Thorax 2008;63 (Suppl IV):iv58.
-
- Schuh S, Macias C, Freedman S, et al. North American practice patterns of IV magnesium therapy in severe acute asthma in children. Acad Emerg Med 2010; 17:1189–1196. - PubMed
-
- Rowe BH. Intravenous and inhaled MgSO4 for acute asthma. Lancet Respir Med 2013; 1:276–277. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
