

Vestibular implantation and longitudinal electrical stimulation of the semicircular canal afferents in human subjects
- PMID: 25652917
- PMCID: PMC4480623
- DOI: 10.1152/jn.00171.2013
Vestibular implantation and longitudinal electrical stimulation of the semicircular canal afferents in human subjects
Abstract
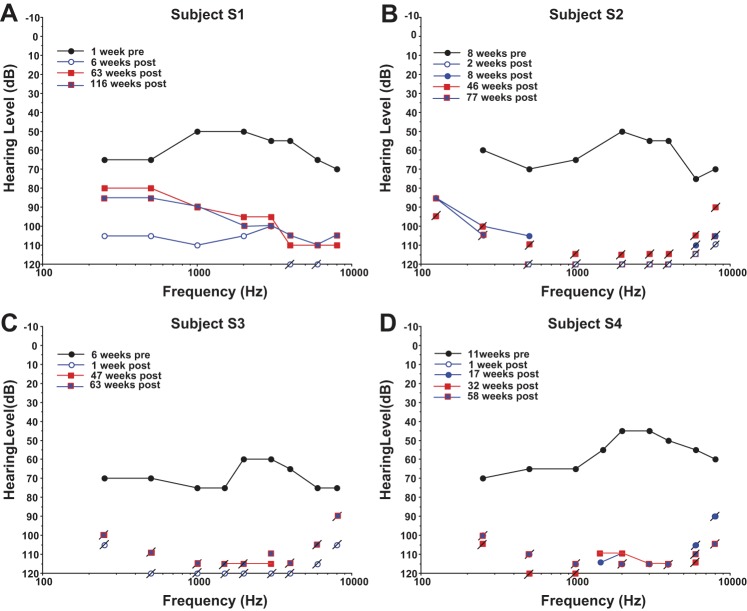
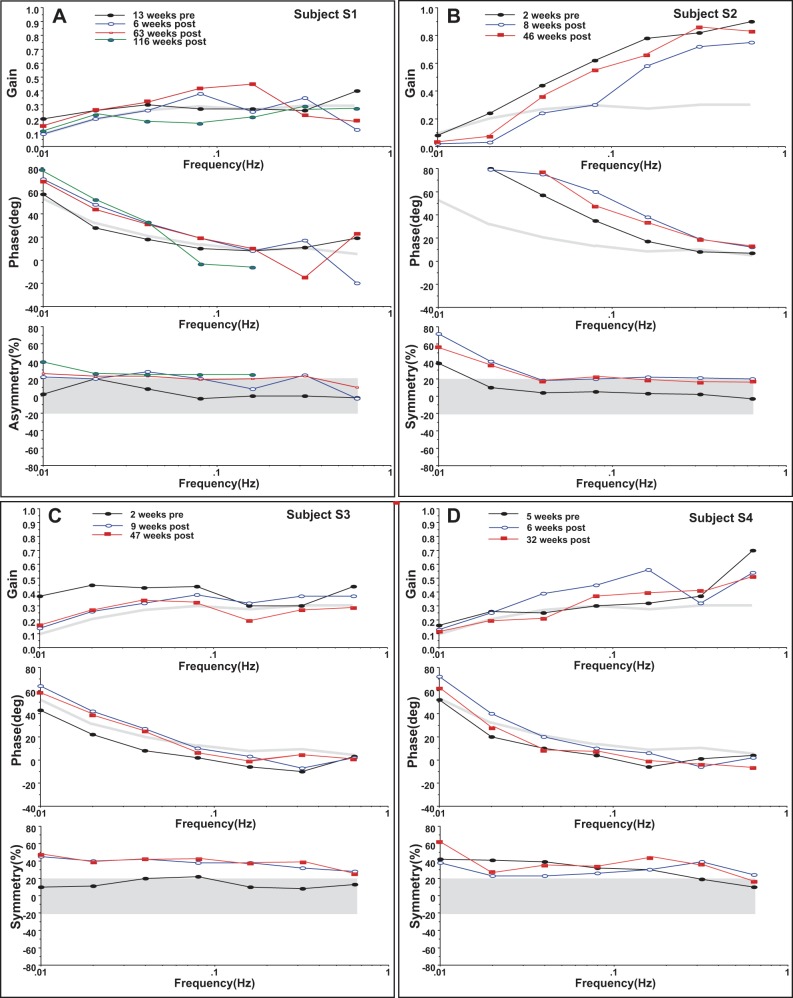
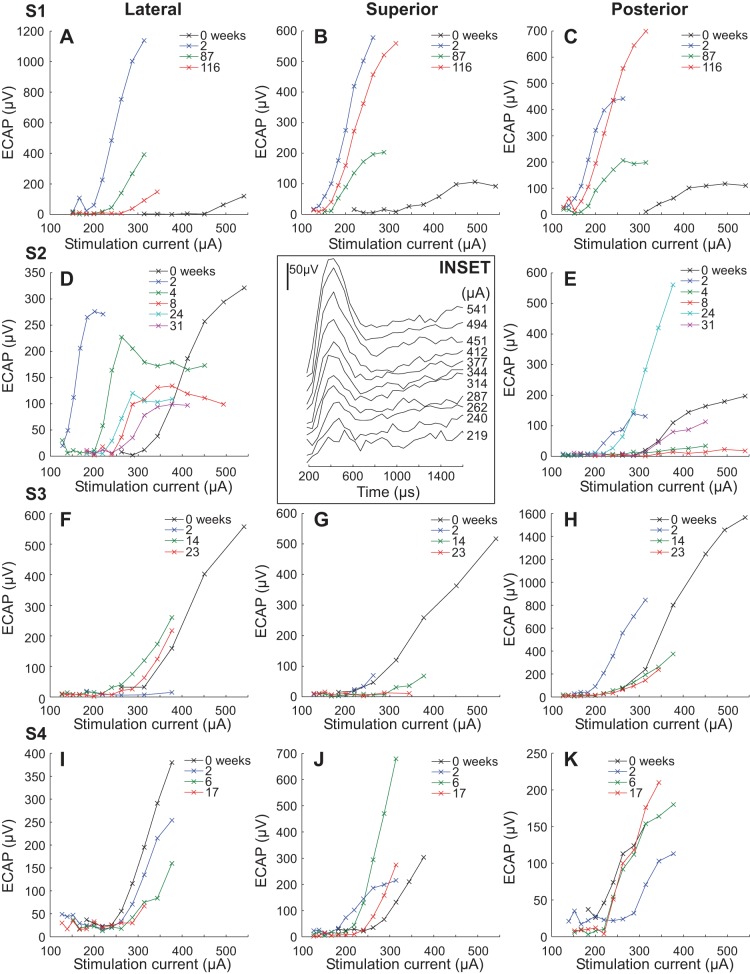
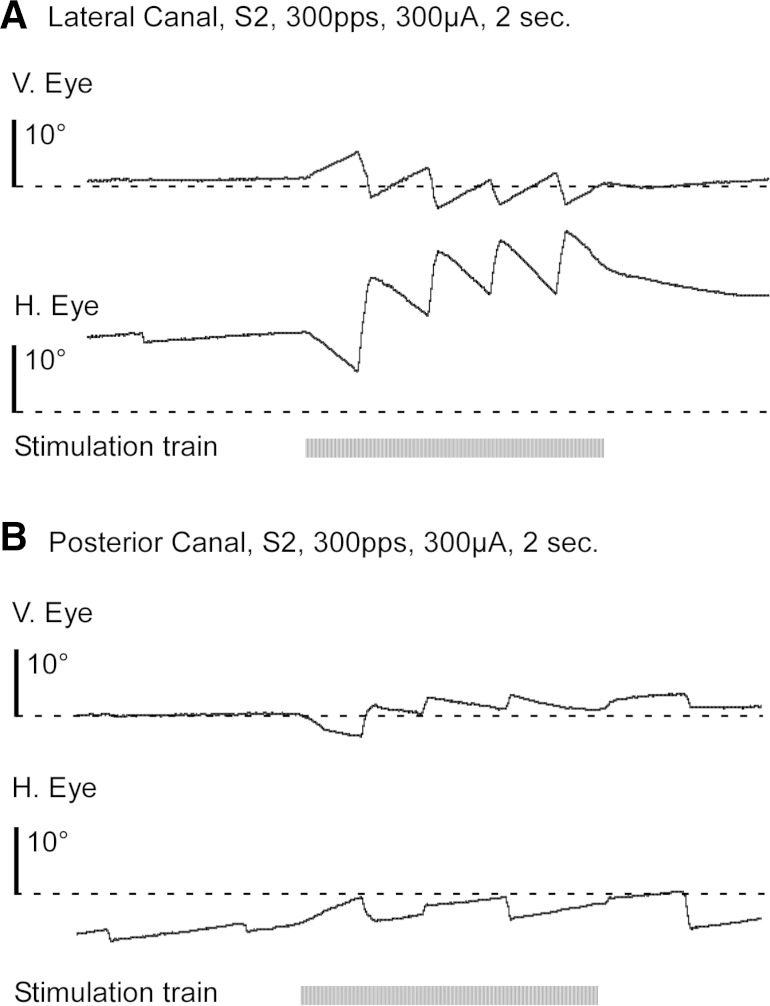
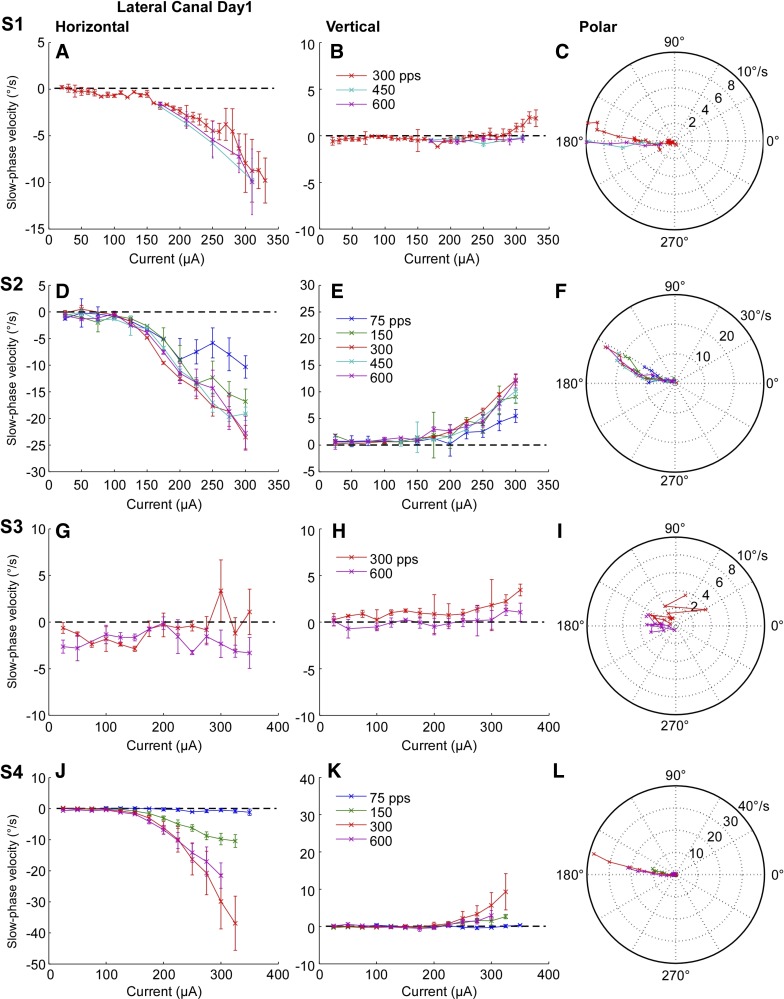
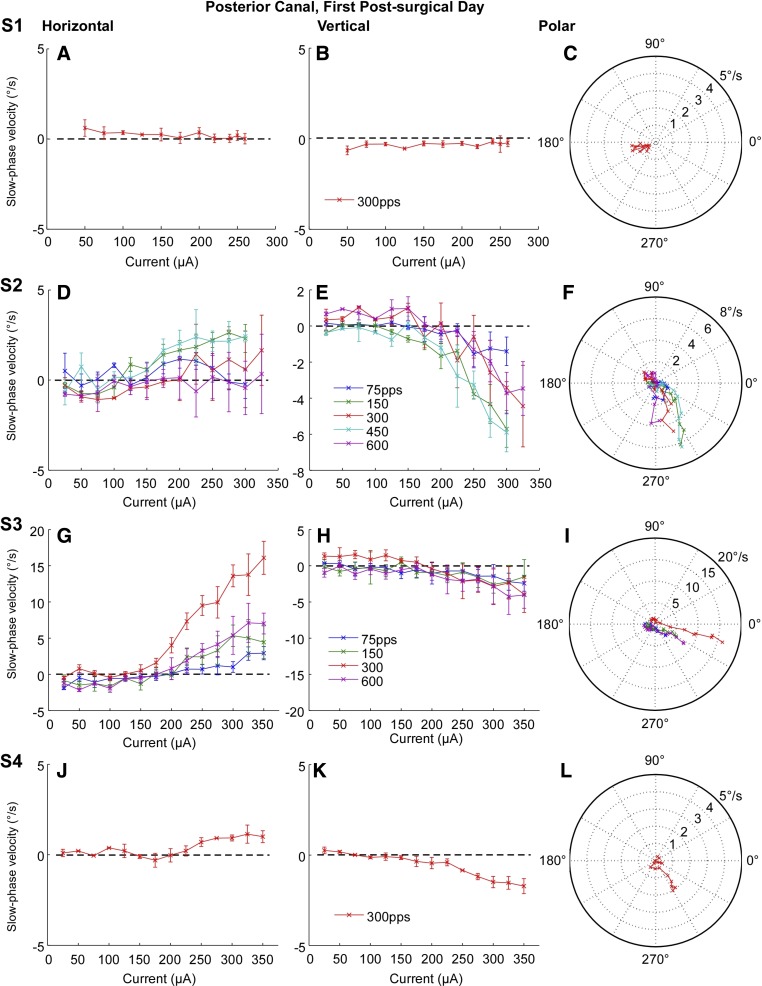
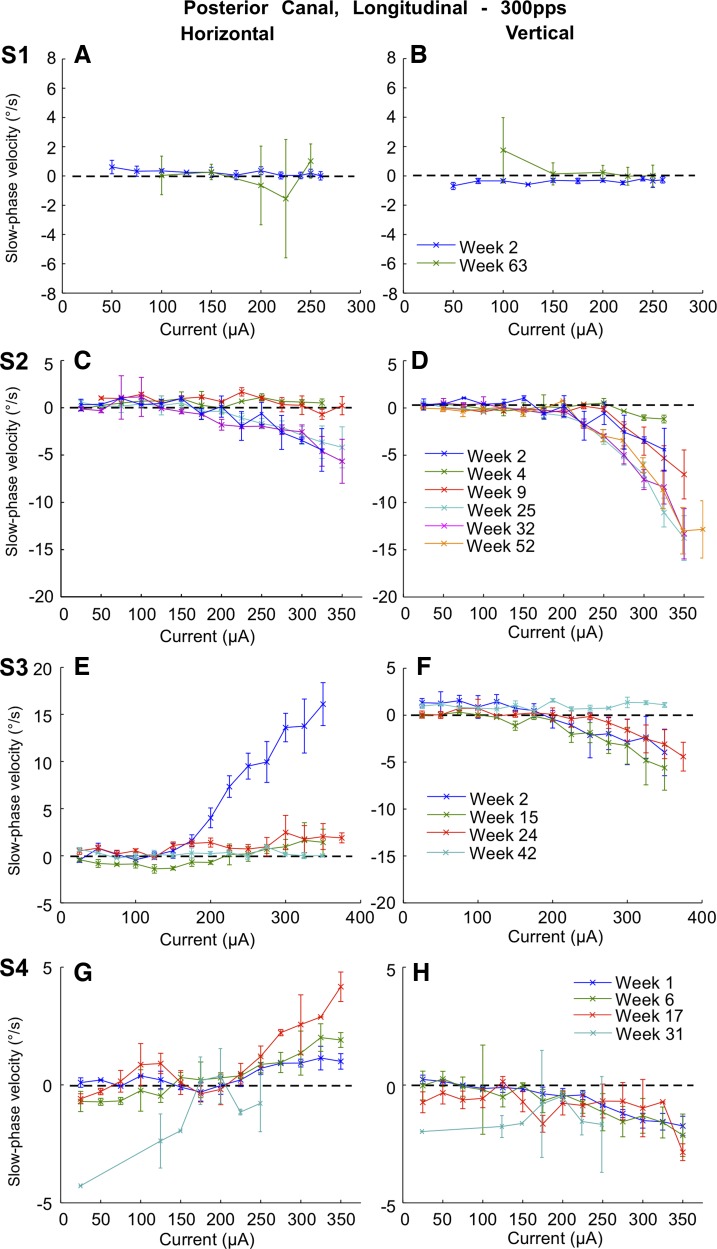
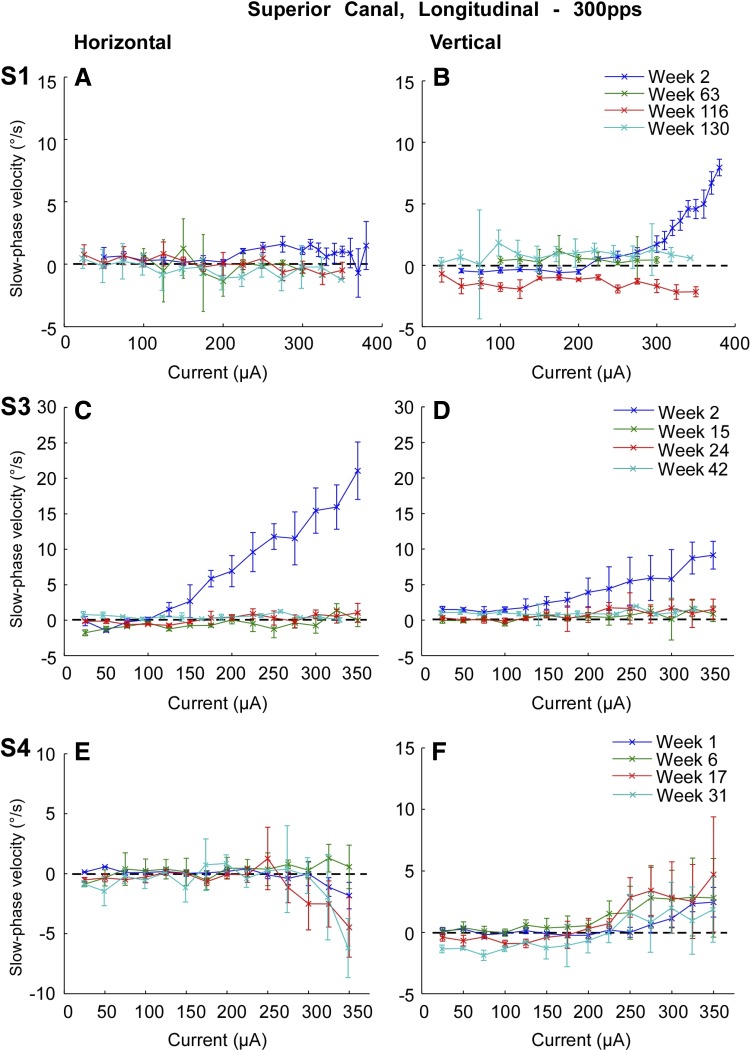
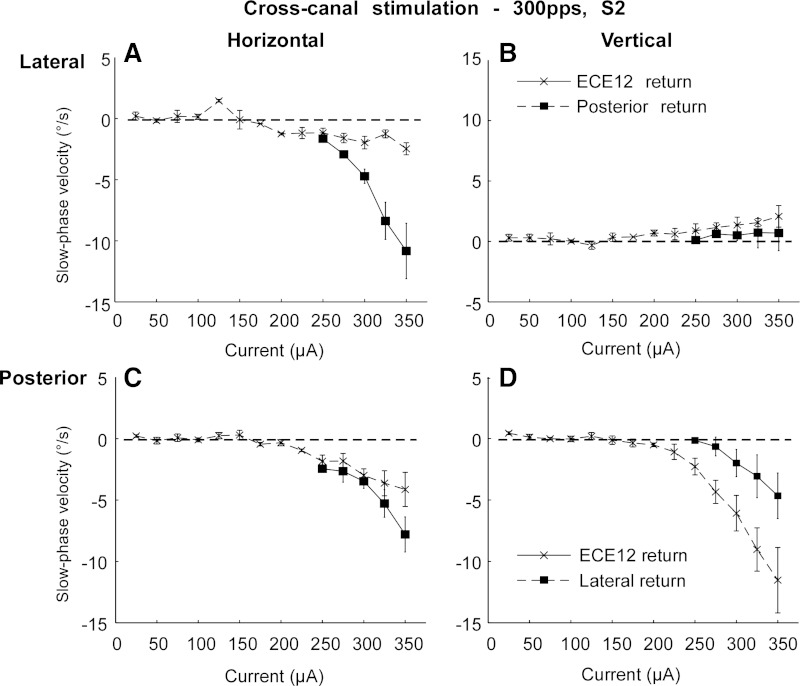
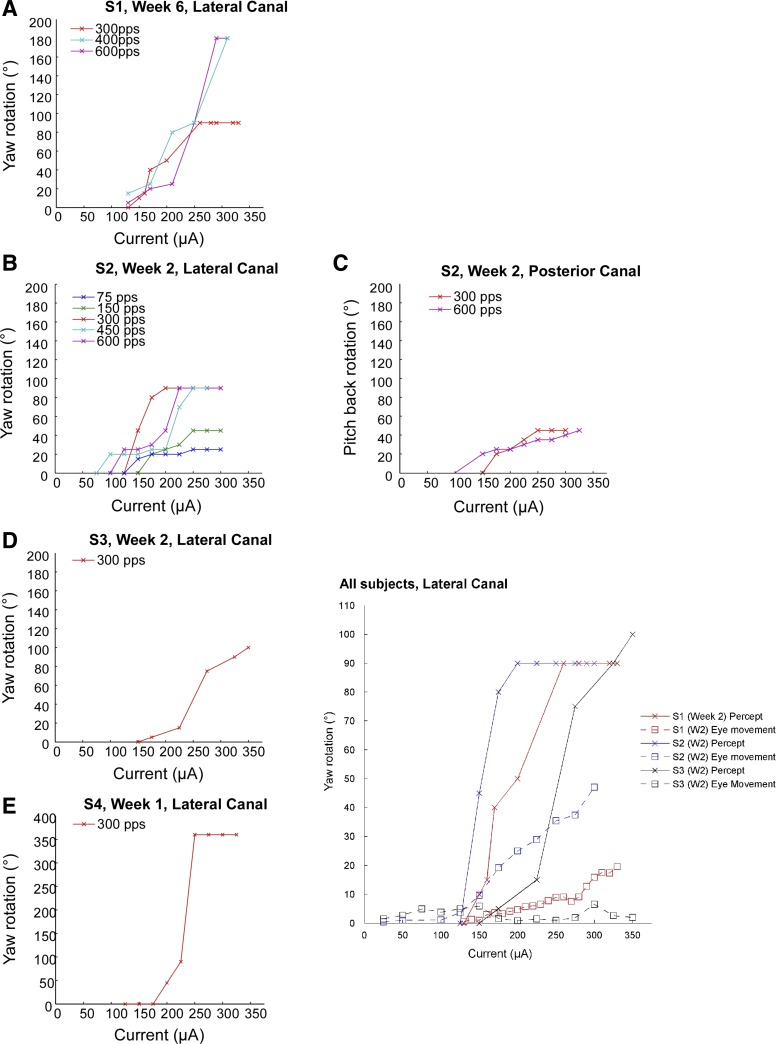
Animal experiments and limited data in humans suggest that electrical stimulation of the vestibular end organs could be used to treat loss of vestibular function. In this paper we demonstrate that canal-specific two-dimensionally (2D) measured eye velocities are elicited from intermittent brief 2 s biphasic pulse electrical stimulation in four human subjects implanted with a vestibular prosthesis. The 2D measured direction of the slow phase eye movements changed with the canal stimulated. Increasing pulse current over a 0-400 μA range typically produced a monotonic increase in slow phase eye velocity. The responses decremented or in some cases fluctuated over time in most implanted canals but could be partially restored by changing the return path of the stimulation current. Implantation of the device in Meniere's patients produced hearing and vestibular loss in the implanted ear. Electrical stimulation was well tolerated, producing no sensation of pain, nausea, or auditory percept with stimulation that elicited robust eye movements. There were changes in slow phase eye velocity with current and over time, and changes in electrically evoked compound action potentials produced by stimulation and recorded with the implanted device. Perceived rotation in subjects was consistent with the slow phase eye movements in direction and scaled with stimulation current in magnitude. These results suggest that electrical stimulation of the vestibular end organ in human subjects provided controlled vestibular inputs over time, but in Meniere's patients this apparently came at the cost of hearing and vestibular function in the implanted ear.
Keywords: Meniere's; human; implant; vestibular.
Copyright © 2015 the American Physiological Society.
Figures




References
-
- Baird RA, Desmadryl G, Fernández C, Goldberg JM. The vestibular nerve of the chinchilla. II. Relation between afferent response properties and peripheral innervation patterns in the semicircular canals. J Neurophysiol 60: 182–203, 1988. - PubMed
-
- Barnett-Cowan M, Harris LR. Perceived timing of vestibular stimulation relative to touch, light, and sound. Exp Brain Res 198: 221–231, 2009. - PubMed
-
- Benson AJ, Spencer MB, Stott JR. Thresholds for the detection of the direction of whole- body, linear movement in the horizontal plane. Aviat Space Environ Med 57: 1088–1096, 1986. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical