

Influence of socioeconomic factors on hospital readmissions for heart failure and acute myocardial infarction in patients 65 years and older: evidence from a systematic review
- PMID: 25653510
- PMCID: PMC4310718
- DOI: 10.2147/CIA.S71165
Influence of socioeconomic factors on hospital readmissions for heart failure and acute myocardial infarction in patients 65 years and older: evidence from a systematic review
Abstract
Purpose: Cardiovascular diseases are the leading cause of death and disability worldwide. Among these diseases, heart failure (HF) and acute myocardial infarction (AMI) are the most common causes of hospitalization. Therefore, readmission for HF and AMI is receiving increasing attention. Several socioeconomic factors could affect readmissions in this target group, and thus, a systematic review was conducted to identify the effect of socioeconomic factors on the risk for readmission in people aged 65 years and older with HF or AMI.
Methods: The search was carried out by querying an electronic database and hand searching. Studies with an association between the risk for readmission and at least one socioeconomic factor in patients aged 65 years or older who are affected by HF or AMI were included. A quality assessment was conducted independently by two reviewers. The agreement was quantified by Cohen's Kappa statistic. The outcomes of studies were categorized in the short-term and the long-term, according to the follow-up period of readmission. A positive association was reported if an increase in the risk for readmission among disadvantaged patients was found. A cumulative effect of socioeconomic factors was computed by considering the association for each study and the number of available studies.
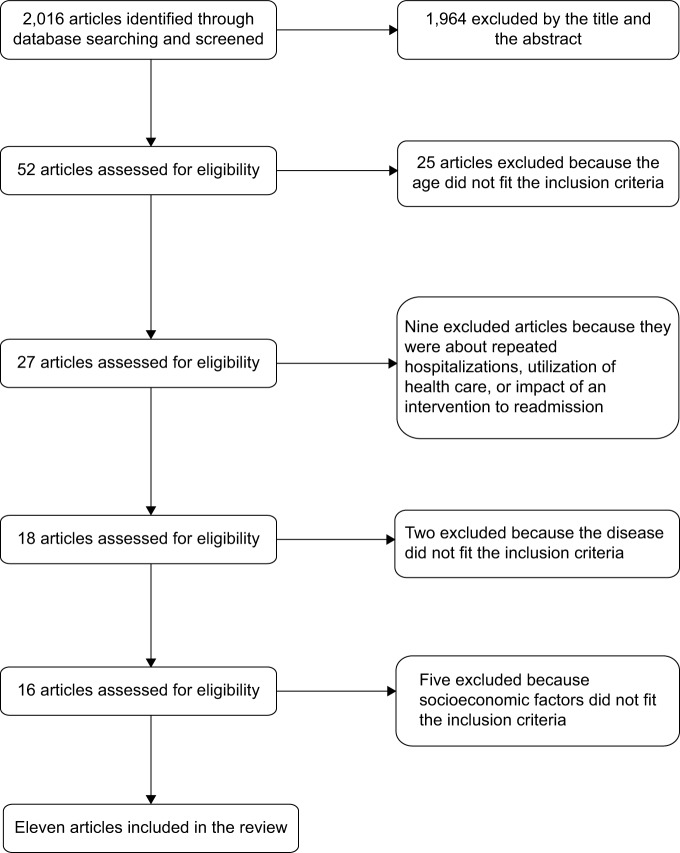
Results: A total of eleven articles were included in the review. They were mainly published in the United States. All the articles analyzed patients who were hospitalized for HF, and four of them also analyzed patients with AMI. Seven studies (63.6%) were found for the short-term outcome, and four studies (36.4%) were found for the long-term outcome. For the short-term outcome, race/ethnicity and marital status showed a positive cumulative effect on the risk for readmission. Regarding the educational level of a patient, no effect was found.
Conclusion: Among the socioeconomic factors, mainly race/ethnicity and marital status affect the risk for readmission in elderly people with HF or AMI. Multidisciplinary hospital-based quality initiatives, disease management, and care transition programs are a priority for health care systems to achieve better coordination.
Keywords: cardiovascular disease (CVD); chronic conditions; disparities; older patients; re-hospitalization; socioeconomic factors.
Figures
References
-
- Organisation for Economic Co-operation and Development . OECD Better Life Index. Paris, France: Organisation for Economic Co-operation and Development; [Accessed July 14, 2014]. Available from: http://www.oecdbetterlifeindex.org/topics/health/
-
- World Health Organization . Chronic Diseases and Health Promotion. Geneva, Switzerland: World Health Organization; [Accessed July 14, 2014]. Available from: http://www.who.int/chp/en/
-
- AARP Public Policy Institute . Chronic Care: A Call to Action for Health Reform. Washington, DC: AARP; 2009. [Accessed July 14, 2014]. Available from: http://assets.aarp.org/rgcenter/health/beyond_50_hcr.pdf.
-
- Courtney M, Edwards H, Chang A, Parker A, Finlayson K, Hamilton K. Fewer emergency readmissions and better quality of life for older adults at risk of hospital readmission: a randomized controlled trial to determine the effectiveness of a 24-week exercise and telephone follow-up program. J Am Geriatr Soc. 2009;57(3):395–402. - PubMed
-
- Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med. 1995;333(18):1190–1195. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
