

Multicenter, prospective, comparative cohort study evaluating the efficacy and safety of alfuzosin 10 mg with regard to blood pressure in men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia with or without antihypertensive medications
- PMID: 25653511
- PMCID: PMC4303366
- DOI: 10.2147/CIA.S74102
Multicenter, prospective, comparative cohort study evaluating the efficacy and safety of alfuzosin 10 mg with regard to blood pressure in men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia with or without antihypertensive medications
Abstract
Background: The objective of this study was to assess the efficacy and safety of alfuzosin 10 mg monotherapy or combined antihypertensive medication on blood pressure (BP) in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia (BPH/LUTS) with or without antihypertensive medication.
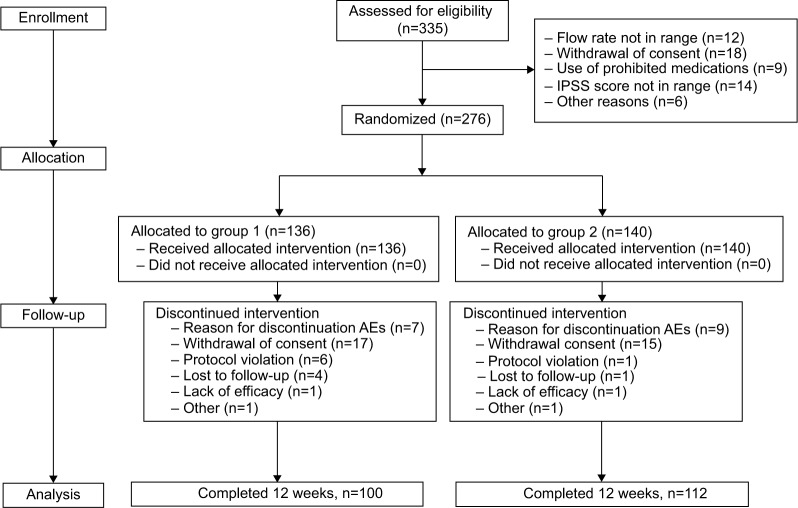
Methods: This was a 3-month, multicenter, randomized, open-label study in 335 patients aged ≥45 years with a clinical diagnosis of BPH/LUTS by medical history and clinical examination, a total International Prostatic Symptom Score (IPSS) ≥8 points, a maximum flow rate >5 mL/sec and ≤15 mL/sec, and a voided volume ≥120 mL. Eligible subjects were randomized to receive alfuzosin 10 mg as monotherapy (group 1) or alfuzosin 10 mg + antihypertensive combination therapy (group 2). Based on baseline BP and hypertensive history with or without antihypertensive medications at first medical examination, group 1 was divided into two subgroups of normotensive and untreated hypertensive patients, and group 2 into two subgroups of controlled hypertensive and uncontrolled hypertensive patients. The primary study outcomes were change in IPSS, BP, and heart rate from baseline. Secondary outcomes were change in IPSS-quality of life score, maximum flow rate, average flow rate, voided volume, and post-voided volume.
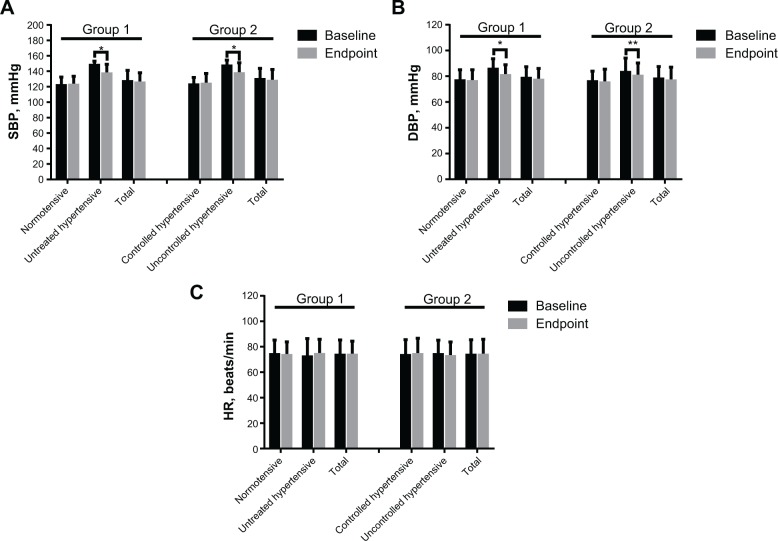
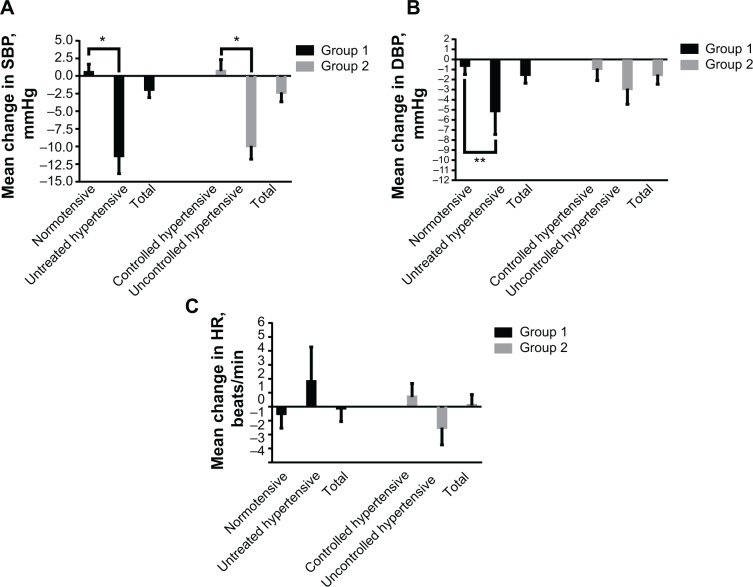
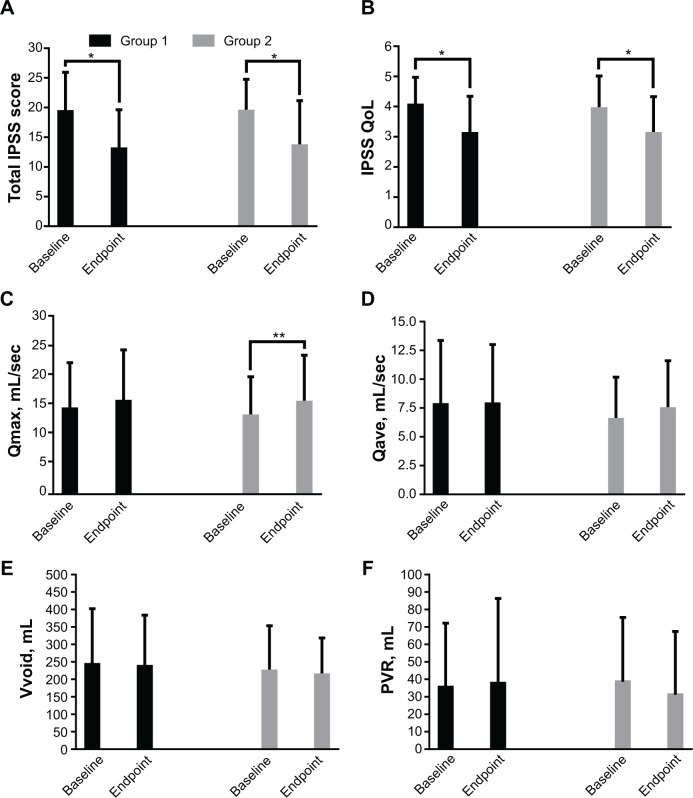
Results: The overall BP change was not significantly different between groups 1 and 2 (systolic BP, P=0.825; diastolic BP, P>0.999). In patients with uncontrolled or untreated hypertension, alfuzosin 10 mg alone or combined with antihypertensive therapy significantly decreased systolic and diastolic BP. The mean difference in total IPSS and IPSS-quality of life scores from baseline between groups 1 and 2 was 0.45 (95% CI: -1.26, 2.16) and 0.12 (95% CI: -0.21, 0.45), respectively (both P>0.05). Maximum flow rate, average flow rate, voided volume, and post-voided volume at endpoint were numerically, but not significantly, changed from baseline (all P>0.05).
Conclusion: This study shows that alfuzosin 10 mg is effective and well tolerated in patients with BPH/LUTS with or without antihypertensive medications. However, in patients with uncontrolled or untreated hypertension, alfuzosin 10 mg alone or in combination with antihypertensive medication appears to decrease systolic and diastolic BP, and these patients should be warned about a decrease in BP on initiation of therapy.
Keywords: alfuzosin; antihypertensive medication; benign prostatic hyperplasia; blood pressure; lower urinary tract symptoms.
Figures
Comment in
-
Personalized therapeutics of α₁-blockers in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia.Clin Interv Aging. 2015 Mar 26;10:621-2. doi: 10.2147/CIA.S82435. eCollection 2015. Clin Interv Aging. 2015. PMID: 25848238 Free PMC article. No abstract available.
-
Authors' reply.Clin Interv Aging. 2015;10:623-4. Clin Interv Aging. 2015. PMID: 25890977 No abstract available.
Similar articles
-
A randomized, comparative, open-label study of efficacy and tolerability of alfuzosin, tamsulosin and silodosin in benign prostatic hyperplasia.Indian J Pharmacol. 2016 Mar-Apr;48(2):134-40. doi: 10.4103/0253-7613.178825. Indian J Pharmacol. 2016. PMID: 27127315 Free PMC article. Clinical Trial.
-
Alfuzosin 10 mg once daily for treating benign prostatic hyperplasia: a 3-year experience in real-life practice.BJU Int. 2008 Apr;101(7):847-52. doi: 10.1111/j.1464-410X.2008.07458.x. BJU Int. 2008. PMID: 18321317
-
Comparison of alfuzosin 10 mg with or without propiverine 10 mg, 20 mg in men with lower urinary tract symptom and an overactive bladder: randomised, single-blind, prospective study.Int J Clin Pract. 2014 Apr;68(4):471-7. doi: 10.1111/ijcp.12339. Epub 2014 Jan 29. Int J Clin Pract. 2014. PMID: 24471868 Clinical Trial.
-
Tadalafil - a therapeutic option in the management of BPH-LUTS.Int J Clin Pract. 2014 Jan;68(1):94-103. doi: 10.1111/ijcp.12305. Int J Clin Pract. 2014. PMID: 24341303 Review.
-
Patients with uncontrolled hypertension or concomitant hypertension and benign prostatic hyperplasia.Clin Cardiol. 2004 Feb;27(2):63-9. doi: 10.1002/clc.4960270203. Clin Cardiol. 2004. PMID: 14979621 Free PMC article. Review.
Cited by
-
Safety and efficacy of tamsulosin, alfuzosin or silodosin as monotherapy for LUTS in BPH - a double-blind randomized trial.Cent European J Urol. 2017 Jun 30;70(2):148-153. doi: 10.5173/ceju.2017.924. Epub 2017 Jun 7. Cent European J Urol. 2017. PMID: 28721281 Free PMC article.
-
Personalized therapeutics of α₁-blockers in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia.Clin Interv Aging. 2015 Mar 26;10:621-2. doi: 10.2147/CIA.S82435. eCollection 2015. Clin Interv Aging. 2015. PMID: 25848238 Free PMC article. No abstract available.
-
Alfuzosin for the medical treatment of benign prostatic hyperplasia and lower urinary tract symptoms: a systematic review of the literature and narrative synthesis.Ther Adv Urol. 2021 Apr 12;13:1756287221993283. doi: 10.1177/1756287221993283. eCollection 2021 Jan-Dec. Ther Adv Urol. 2021. PMID: 33912246 Free PMC article. Review.
References
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Garraway WM, Collins GN, Lee RJ. High prevalence of benign prostatic hypertrophy in the community. Lancet. 1991;338:469–471. - PubMed
-
- McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–1803. - PubMed
-
- Madersbacher S, Alivizatos G, Nordling J, et al. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines) Eur Urol. 2004;46:547–554. - PubMed
-
- McVary KT. Alfuzosin for symptomatic benign prostatic hyperplasia: long-term experience. J Urol. 2006;175:35–42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
