

Home-based telehealth hospitalization for exacerbation of chronic obstructive pulmonary disease: findings from "the virtual hospital" trial
- PMID: 25654366
- PMCID: PMC4432494
- DOI: 10.1089/tmj.2014.0098
Home-based telehealth hospitalization for exacerbation of chronic obstructive pulmonary disease: findings from "the virtual hospital" trial
Abstract
Background: Telehealth interventions for patients with chronic obstructive pulmonary disease (COPD) have focused primarily on stable outpatients. Telehealth designed to handle the acute exacerbation that normally requires hospitalization could also be of interest. The aim of this study was to compare the effect of home-based telehealth hospitalization with conventional hospitalization for exacerbation in severe COPD.
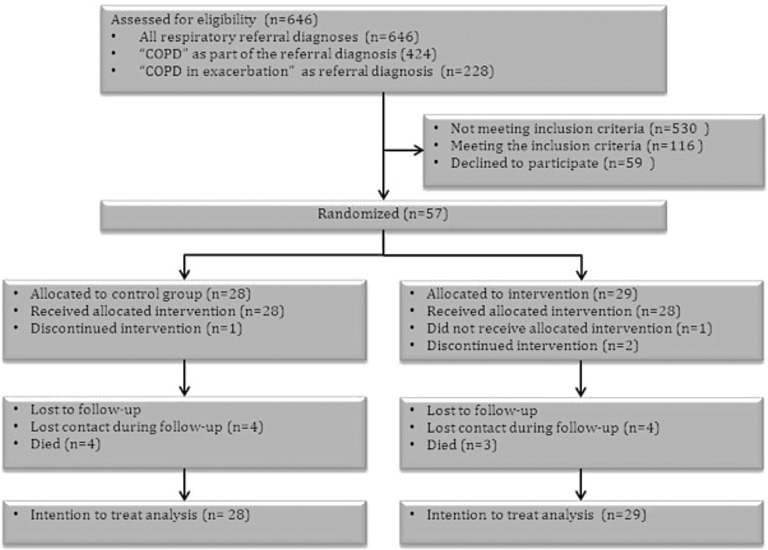
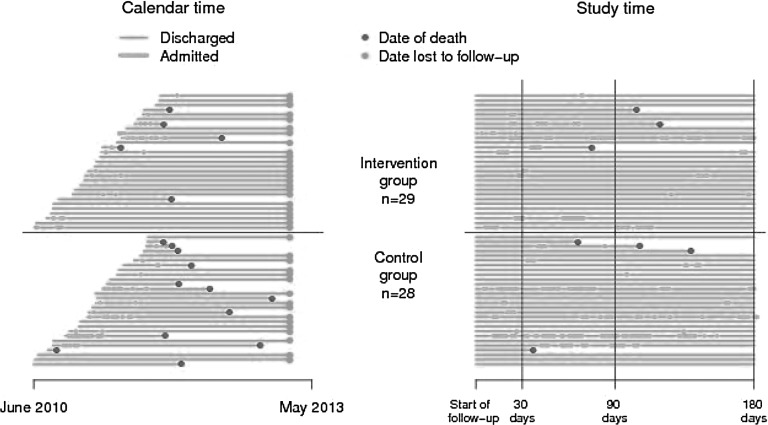
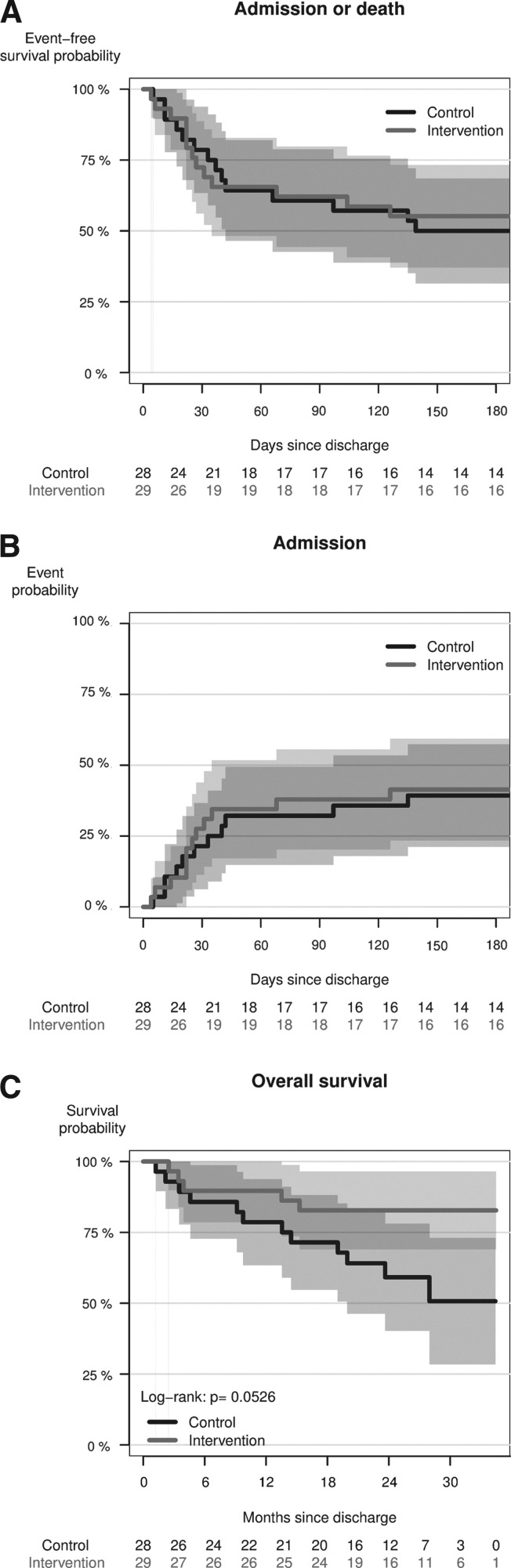
Materials and methods: A two-center, noninferiority, randomized, controlled effectiveness trial was conducted between June 2010 and December 2011. Patients with severe COPD admitted because of exacerbation were randomized 1:1 either to home-based telehealth hospitalization or to continue standard treatment and care at the hospital. The primary outcome was treatment failure defined as re-admission due to exacerbation in COPD within 30 days after initial discharge. The noninferiority margin was set at 20% of the control group's risk of re-admission. Secondary outcomes were mortality, need for manual or mechanical ventilation or noninvasive ventilation, length of hospitalization, physiological parameters, health-related quality of life, user satisfaction, healthcare costs, and adverse events.
Results: In total, 57 patients were randomized: 29 participants in the telehealth group and 28 participants in the control group. Testing the incidence of re-admission within 30 days after discharge could not confirm noninferiority (lower 95% confidence limit [CL], -24.8%; p=0.35). Results were also nonsignificant at 90 days (lower 95% CL, -16.2%; p=0.33) and 180 days (lower 95% CL, -16.6%; p =0.33) after discharge. Superiority testing on secondary outcomes showed nonsignificant differences between groups. Healthcare costs have not yet been evaluated.
Conclusions: Whether home-based telehealth hospitalization is noninferior to conventional hospitalization requires further investigation. The results indicate that a subgroup of patients with severe COPD can be treated for acute exacerbation at home using telehealth, without the physical presence of health professionals and with a proper organizational "back-up."
Keywords: home health monitoring; telehealth; telemedicine; telenursing.
Figures

References
-
- Sundhedsstyrelsen, Monitorering & Medicinsk Teknologivurdering. Genindlæggelser af ældre i Danmark 2008—Nye tal fra Sundhedsstyrelsen. 2009. Available at www.sst.dk/publ/Publ2009/DOKU/nye_tal/Genindlaeggelser2008_final_uden_bi... (last accessed February24, 2014)
-
- Teknologirådet. Sundhedsydelser med IT—Pervasive HealthCare i den danske sundhedssektor. Vurderinger og anbefalinger fra en arbejdsgruppe under Teknologirådet. 2006. Available at www.tekno.dk/pdf/projekter/p06_pervasive-healthcare.pdf (last accessed February24, 2014)
-
- Bolton CE, Waters CS, Peirce S, Elwyn G; EPSRC and MRC Grand ChallengeTeam. Insufficient evidence of benefit: A systematic review of home telemonitoring for COPD. J Eval Clin Pract 2011;17:1216–1222 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
