

Surveillance of moderate-size aneurysms of the thoracic aorta
- PMID: 25655070
- PMCID: PMC4331418
- DOI: 10.1186/s13019-015-0220-2
Surveillance of moderate-size aneurysms of the thoracic aorta
Abstract
Background: There are no evidence based guidelines for the surveillance of patients with moderate-sized (<5 cm) thoracic aortic aneurysms (MTAA), who do not warrant surgical intervention. The purpose of this study was to review the MTAA patient surveillance strategy used currently at the Northport Veterans Affairs Medical Center, to assess outcomes over time and accrue data to develop guidelines to optimize MTAA patients' follow-up.
Methods: The study group included veterans referred to the Thoracic Surgery clinic for the management of moderate-sized (<5 cm) thoracic aortic aneurysms (MTAA) not warranting immediate surgical repair. As a pilot study, all MTAA patients' charts from 2005-2013 were reviewed to describe imaging practices and evaluate patient-specific long-term outcomes. An adverse composite endpoint was defined if a patient's aneurysm grew substantially (≥0.5 cm/year or reached 5.5 cm) or a MTAA-related event (surgery or death) occurred. Additionally, number of CT scans obtained during the follow up period were documented.
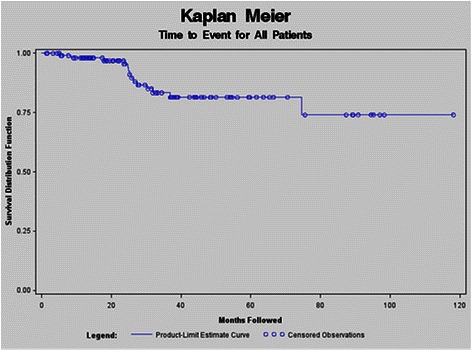
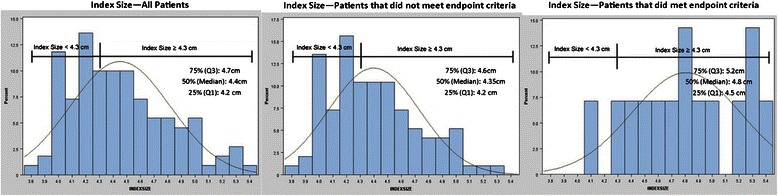
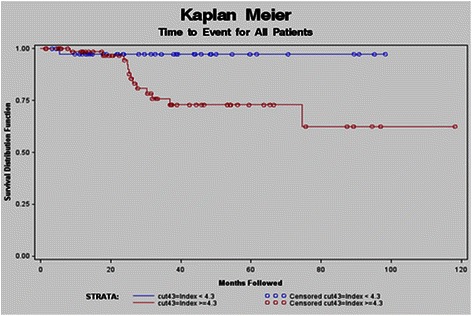
Results: For 110 MTAA patients, the average presenting index size was 4.45 ± 0.4 cm with average growth of 0.04 cm total (0.03 cm/year). Fourteen (13%) patients met the adverse composite endpoint, with no MTAA-related deaths. Patients achieving the adverse composite endpoint had higher index sizes (4.81 vs. 4.40 cm, p = 0.001) and higher average growth rates as compared to non-endpoint patients (0.16 vs. 0.01 cm, p = 0.0009). Optimizing the negative likelihood ratio defined a new "not-at-risk" population with aneurysm index size < 4.3 cm. A shorter time to adverse event for "at-risk" patients was found versus "not-at-risk" patients (p = 0.02). On average, there were 4.8 CT scans/patient and estimated cumulative radiation dose of 34 mSv/patient. Only one "not-at-risk" patient had substantive MTAA growth (≥0.5 cm/year) over the 8 year follow-up period.
Conclusion and relevance: Annual imaging of MTAA "not-at-risk" patients appears unwarranted, resulting in potentially excessive radiation exposure. Although additional research is necessary for validation, longer surveillance imaging intervals (beyond one year) seem appropriate for MTAA patients presenting with < 4.3 cm index aneurysms.
Figures
References
-
- Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27–129. doi: 10.1016/j.jacc.2010.02.015. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
