

Physical Therapist Treatment of Patients in the Neurological Intensive Care Unit: Description of Practice
- PMID: 25655880
- PMCID: PMC4498141
- DOI: 10.2522/ptj.20140112
Physical Therapist Treatment of Patients in the Neurological Intensive Care Unit: Description of Practice
Abstract
Background: Although studies have established the safety and feasibility of physical therapy in the critical care setting, minimal information about physical therapist practice in the neurological intensive care unit (NICU) is available.
Objective: This study describes physical therapists' treatment of people admitted to a NICU.
Design: People admitted to the NICU with a diagnosis of subarachnoid hemorrhage, subdural hematoma, intracranial hemorrhage, or trauma were retrospectively studied.
Methods: Data on patient demographics, use of mechanical ventilation, and intracranial pressure (ICP) monitoring were collected. For each physical therapy session, the length of the session, the location (NICU or post-NICU setting), and the presence of mechanical ventilation or ICP monitoring were recorded. Data on safety parameters, including vital sign response, falls, and dislodgement of lines, were collected.
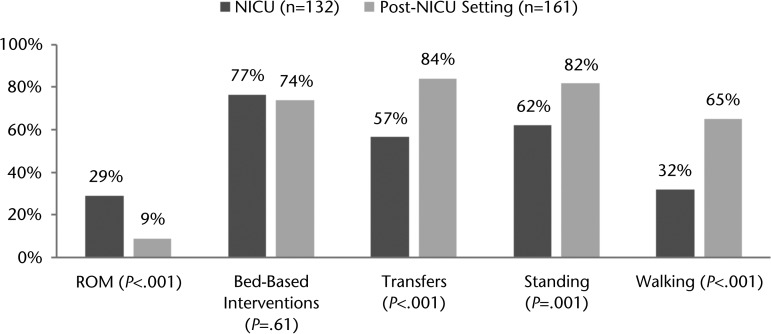
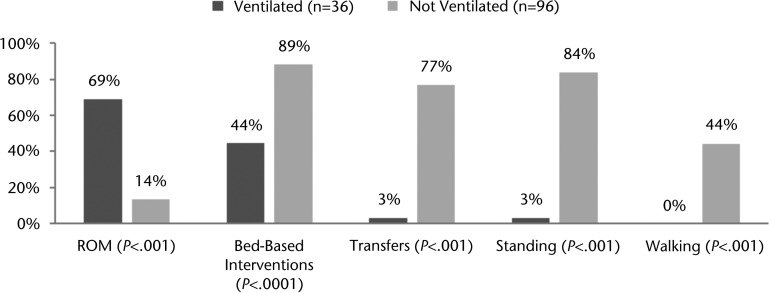
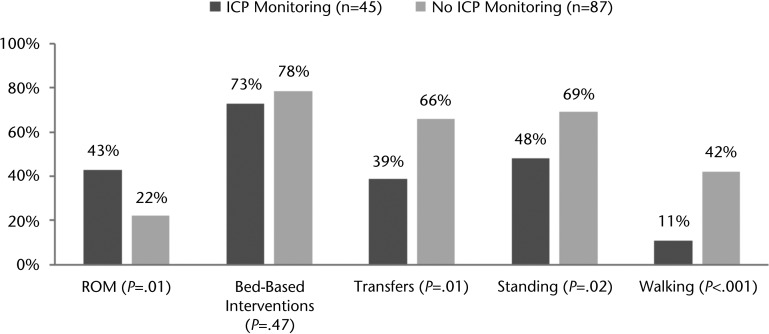
Results: Over 1 year, 180 people were admitted to the NICU; 86 were evaluated by a physical therapist, for a total of 293 physical therapy sessions in the NICU (n=132) or post-NICU setting (n=161). Only one session (0.3%) was stopped, secondary to an increase in ICP. The first physical therapy session occurred on NICU day 3.0 (25%-75% interquartile range=2.0-6.0). Patients received a median of 3.4 sessions per week (25%-75% interquartile range=1.8-5.9). Patients with mechanical ventilation received less frequent physical therapy sessions than those without mechanical ventilation. Patients with ICP monitoring received less frequent sessions than those without ICP monitoring. However, after multivariate analysis, only the admission Glasgow Coma Score was independently associated with physical therapy frequency in the NICU. Patients were more likely to stand, transfer, and walk in the post-NICU setting than in the NICU.
Limitations: The results are limited by the retrospective, single-center nature of the study. There is inherent bias of evaluating only those patients who had physical therapy, and therapists were unable to completely adjust for the severity of illness of a given patient.
Conclusions: Physical therapy was performed safely in the NICU. Patients who required invasive support received less frequent physical therapy.
© 2015 American Physical Therapy Association.
Figures
References
-
- Morris PE, Herridge MS. Early intensive care unit mobility: future directions. Crit Care Clin. 2007;23:97–110. - PubMed
-
- Garzon-Serrano J, Ryan C, Waak K, et al. Early mobilization in critically ill patients: patients' mobilization level depends on health care provider's profession. PM&R. 2011;3:307–313. - PubMed
-
- Li Z, Peng X, Zhu B, et al. Active mobilization for mechanically ventilated patients: a systematic review. Arch Phys Med Rehabil. 2013;94:551–561. - PubMed
-
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007;369:306–318. - PubMed
-
- Kitchener N, Hashem S, Wahba M, et al. Critical Care in Neurology. Flying Publisher & Kamps; 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
