

Visceral leishmaniasis diagnosis and reporting delays as an obstacle to timely response actions in Nepal and India
- PMID: 25656298
- PMCID: PMC4335691
- DOI: 10.1186/s12879-015-0767-5
Visceral leishmaniasis diagnosis and reporting delays as an obstacle to timely response actions in Nepal and India
Abstract
Background: To eliminate visceral leishmaniasis (VL) in India and Nepal, challenges of VL diagnosis, treatment and reporting need to be identified. Recent data indicate that VL is underreported and patients face delays when seeking treatment. Moreover, VL surveillance data might not reach health authorities on time. This study quantifies delays for VL diagnosis and treatment, and analyses the duration of VL reporting from district to central health authorities in India and Nepal.
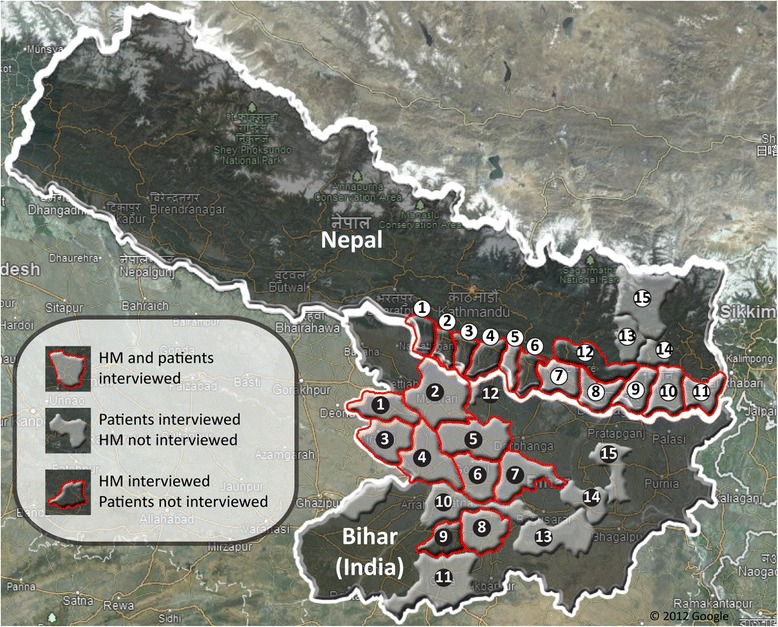
Methods: A cross-sectional study conducted in 12 districts of Terai region, Nepal, and 9 districts of Bihar State, India, in 2012. Patients were interviewed in hospitals or at home using a structured questionnaire, health managers were interviewed at their work place using a semi-structured questionnaire and in-depth interviews were conducted with central level health managers. Reporting formats were evaluated. Data was analyzed using two-tailed Mann-Whitney U or Fisher's exact test.
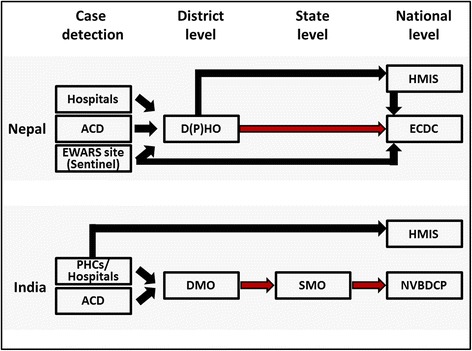
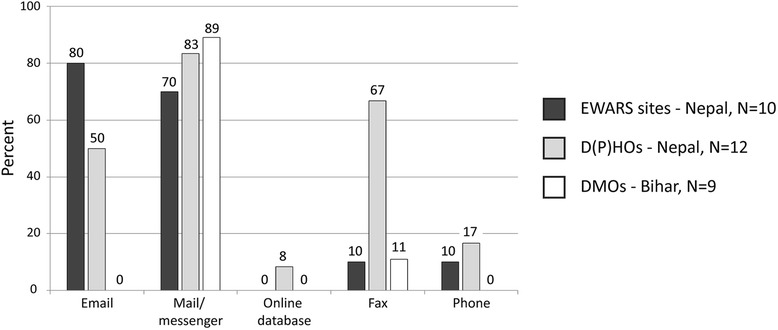
Results: 92 VL patients having experienced 103 VL episodes and 49 district health managers were interviewed. Patients waited in Nepal 30 days (CI 18-42) before seeking health care, 3.75 times longer than in Bihar (8d; CI 4-12). Conversely, the lag time from seeking health care to receiving a VL diagnosis was 3.6x longer in Bihar (90d; CI 68-113) compared to Nepal (25d; CI 13-38). The time span between diagnosis and treatment was short in both countries. VL reporting time was in Nepal 19 days for sentinel sites and 76 days for "District Public Health Offices (DPHOs)". In Bihar it was 28 days for "District Malaria Offices". In Nepal, 73% of health managers entered data into computers compared to 16% in Bihar. In both countries reporting was mainly paper based and standardized formats were rarely used.
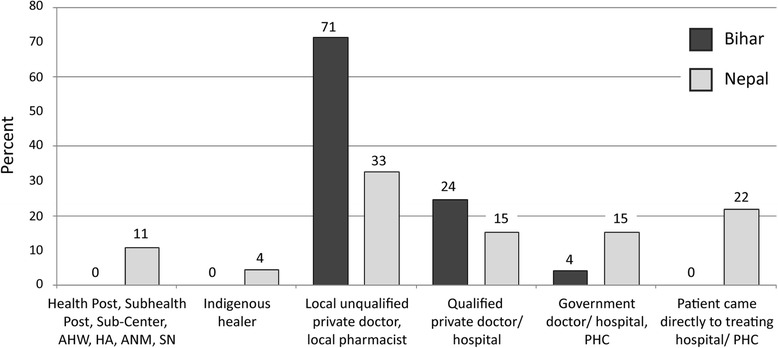
Conclusions: To decrease the delay between onset of symptoms and getting a proper diagnosis and treatment the approaches in the two countries vary: In Nepal health education for seeking early treatment are needed while in Bihar the use of private and non-formal practitioners has to be discouraged. Reinforcement of VL sentinel reporting in Bihar, reorganization of DPHOs in Nepal, introduction of standardized reporting formats and electronic reporting should be conducted in both countries.
Figures

References
-
- WHO Regional Office for South-East Asia, Regional Technical Advisory Group (RTAG) on Kala-azar Elimination . Meeting reports. New Delhi, India: WHO SEARO; 2009. Report of the Third RTAG Meeting.
-
- WHO Regional Office for South-East Asia, Regional Technical Advisory Group (RTAG) on Kala-azar Elimination . Meeting reports. New Delhi, India: WHO SEARO; 2011. Report of the Fourth RTAG Meeting.
-
- Joshi A, Narain JP, Prasittisuk C, Bhatia R, Hashim G, Jorge A, et al. Can visceral leishmaniasis be eliminated from Asia? J Vector Borne Dis. 2008;45(2):105–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
