

Trajectories of risk after hospitalization for heart failure, acute myocardial infarction, or pneumonia: retrospective cohort study
- PMID: 25656852
- PMCID: PMC4353309
- DOI: 10.1136/bmj.h411
Trajectories of risk after hospitalization for heart failure, acute myocardial infarction, or pneumonia: retrospective cohort study
Abstract
Objective: To characterize the absolute risks for older patients of readmission to hospital and death in the year after hospitalization for heart failure, acute myocardial infarction, or pneumonia.
Design: Retrospective cohort study.
Setting: 4767 hospitals caring for Medicare fee for service beneficiaries in the United States, 2008-10.
Participants: More than 3 million Medicare fee for service beneficiaries, aged 65 years or more, surviving hospitalization for heart failure, acute myocardial infarction, or pneumonia.
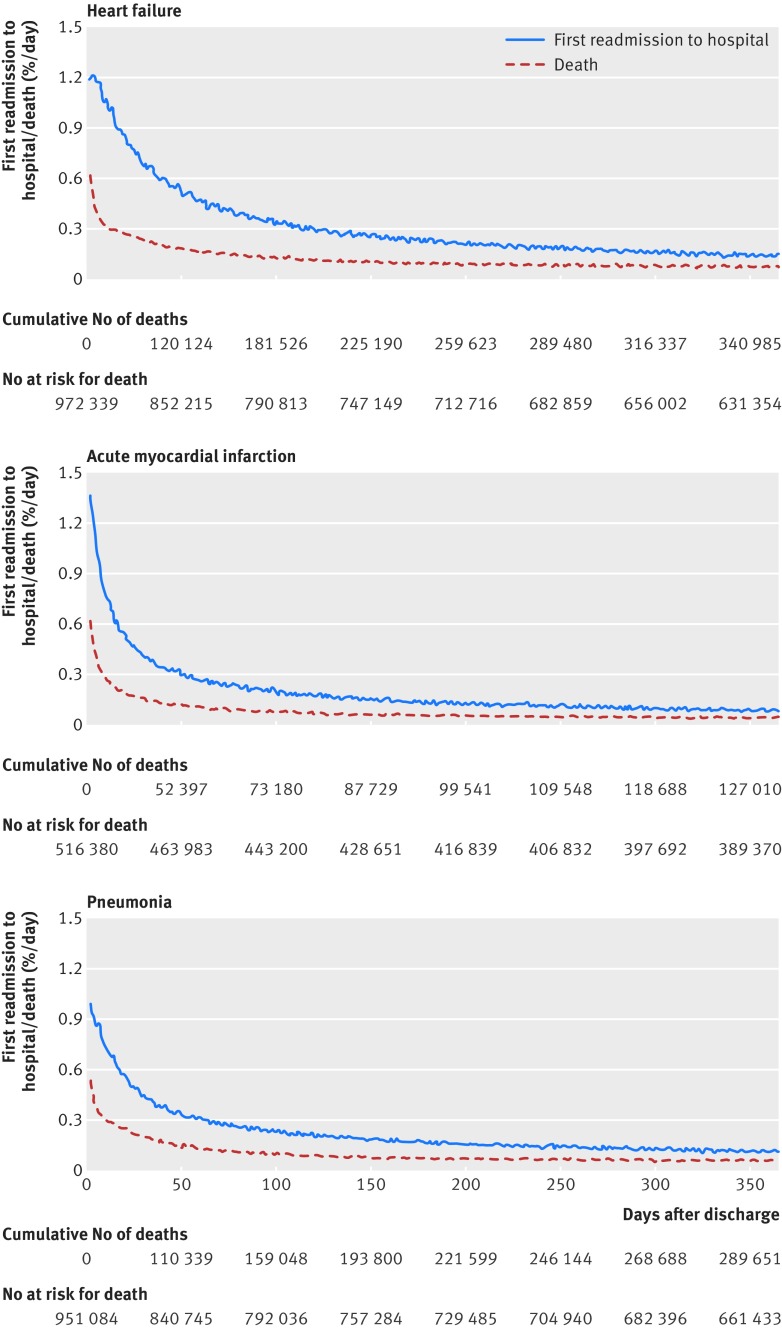
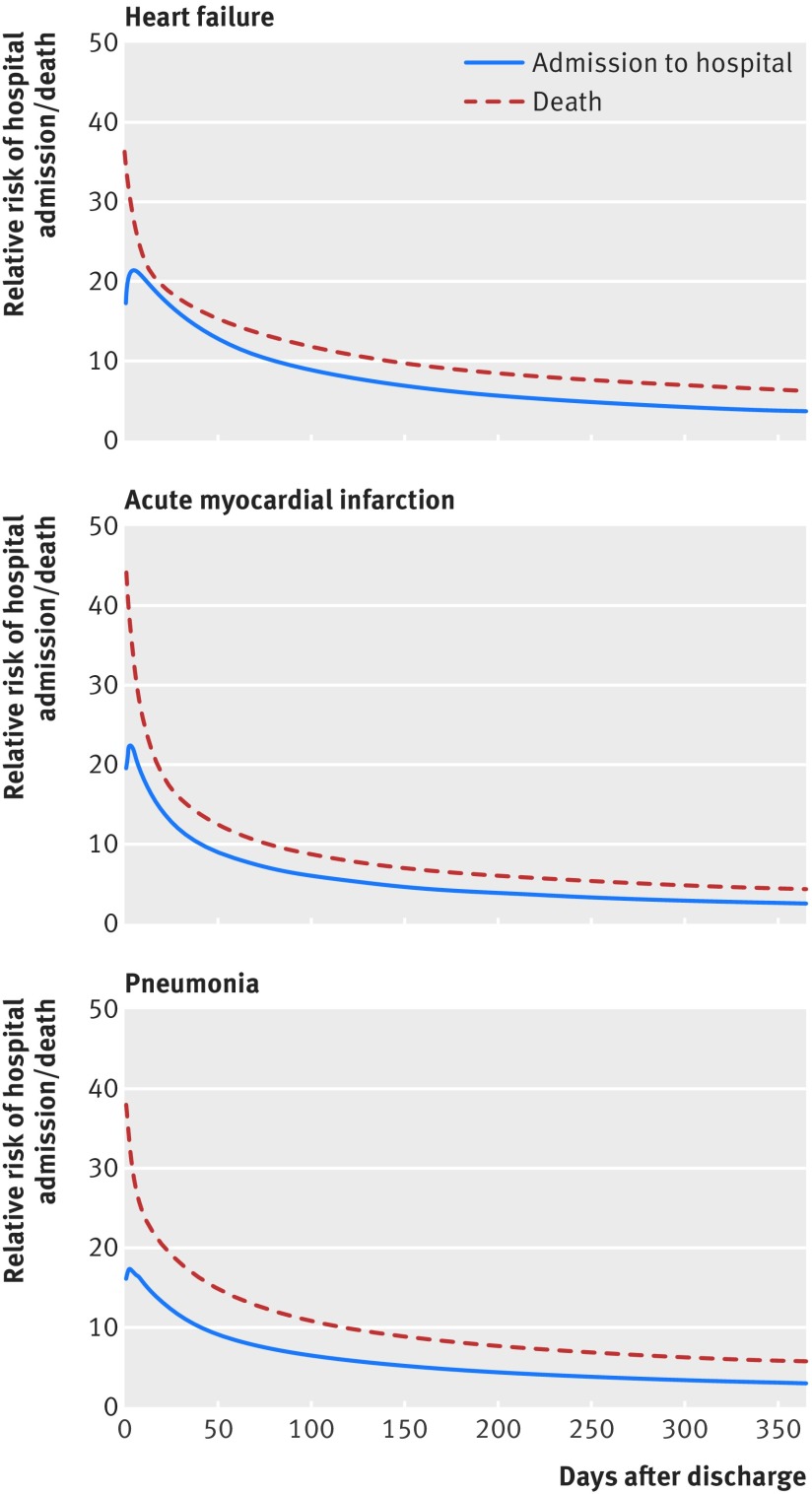
Main outcome measures: Daily absolute risks of first readmission to hospital and death for one year after discharge. To illustrate risk trajectories, we identified the time required for risks of readmission to hospital and death to decline 50% from maximum values after discharge; the time required for risks to approach plateau periods of minimal day to day change, defined as 95% reductions in daily changes in risk from maximum daily declines after discharge; and the extent to which risks are higher among patients recently discharged from hospital compared with the general elderly population.
Results: Within one year of hospital discharge, readmission to hospital and death, respectively, occurred following 67.4% and 35.8% of hospitalizations for heart failure, 49.9% and 25.1% for acute myocardial infarction, and 55.6% and 31.1% for pneumonia. Risk of first readmission had declined 50% by day 38 after hospitalization for heart failure, day 13 after hospitalization for acute myocardial infarction, and day 25 after hospitalization for pneumonia; risk of death declined 50% by day 11, 6, and 10, respectively. Daily change in risk of first readmission to hospital declined 95% by day 45, 38, and 45; daily change in risk of death declined 95% by day 21, 19, and 21. After hospitalization for heart failure, acute myocardial infarction, or pneumonia, the magnitude of the relative risk for hospital admission over the first 90 days was 8, 6, and 6 times greater than that of the general older population; the relative risk of death was 11, 8, and 10 times greater.
Conclusions: Risk declines slowly for older patients after hospitalization for heart failure, acute myocardial infarction, or pneumonia and is increased for months. Specific risk trajectories vary by discharge diagnosis and outcome. Patients should remain vigilant for deterioration in health for an extended time after discharge. Health providers can use knowledge of absolute risks and their changes over time to better align interventions designed to reduce adverse outcomes after discharge with the highest risk periods for patients.
© Dharmarajan et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009;360:1418-28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical