

The role of smoking status on the progression-free survival of non-small cell lung cancer patients harboring activating epidermal growth factor receptor (EGFR) mutations receiving first-line EGFR tyrosine kinase inhibitor versus platinum doublet chemotherapy: a meta-analysis of prospective randomized trials
- PMID: 25657199
- PMCID: PMC4350797
- DOI: 10.1634/theoncologist.2014-0285
The role of smoking status on the progression-free survival of non-small cell lung cancer patients harboring activating epidermal growth factor receptor (EGFR) mutations receiving first-line EGFR tyrosine kinase inhibitor versus platinum doublet chemotherapy: a meta-analysis of prospective randomized trials
Abstract
Background: Univariate analyses from several randomized phase III trials seemed to suggest ever-smokers with advanced mutated epidermal growth factor receptor (EGFRm) non-small cell lung cancer (NSCLC) did not seem to benefit from EGFR tyrosine kinase inhibitors (TKIs) as first-line treatment when compared with platinum-doublet chemotherapy as measured by progression-free survival (PFS).
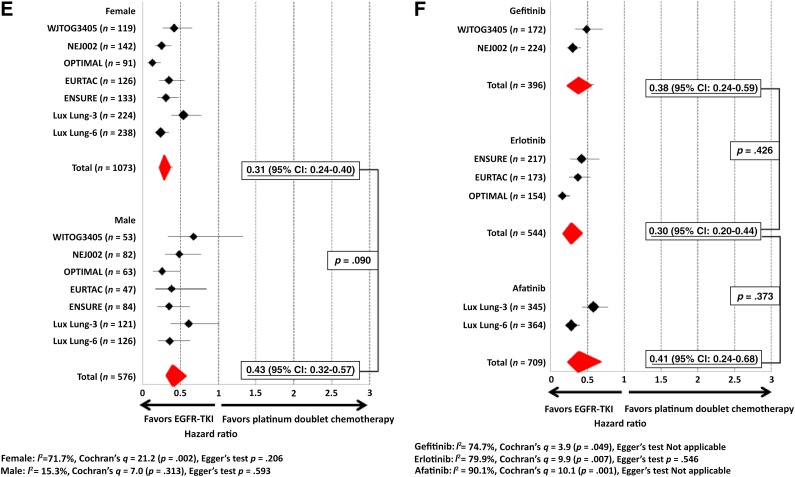
Methods: A literature-based meta-analysis of PFS outcomes as measured by log-transformed pooled hazard ratio (HR) was performed using a random-effect model. Pooled HRs for smoking status, age, gender, ethnicity, type of EGFR mutation, and EGFR TKI were obtained. Comparison of the pooled HR was performed by metaregression analysis.
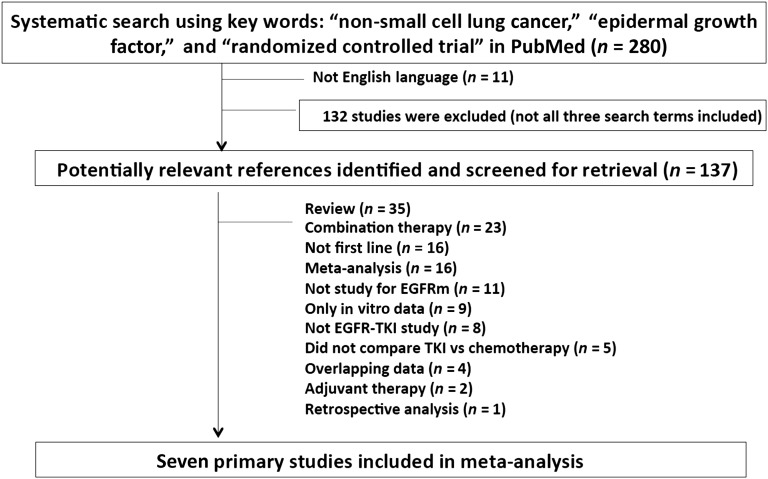
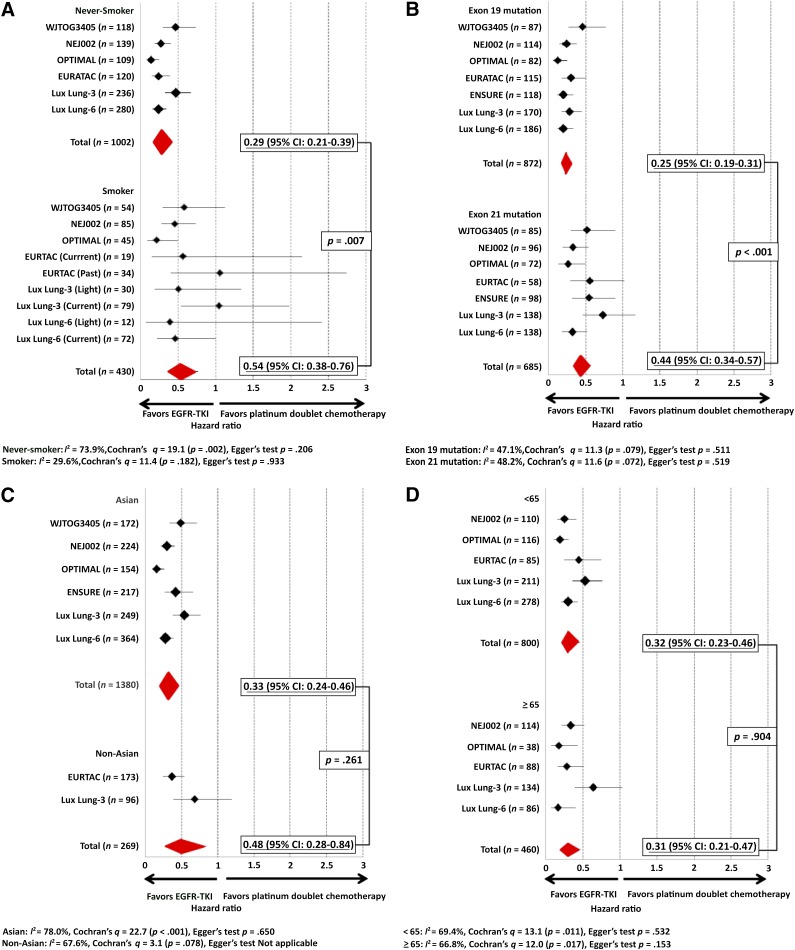
Results: Among the 1,649 EGFRm NSCLC patients analyzed from 7 prospective randomized trials (WJTOG3405, NEJ002, EURTAC, OPTIMAL, LUX Lung-3, LUX Lung-6, and ENSURE), 83.7% were Asians, and 30.0% were ever-smokers. An equal percentage of ever-smokers received doublet chemotherapy (30.2%) or EGFR TKI (30.0%). The pooled HR for PFS was 0.29 (95% confidence interval [CI]: 0.21-0.39) for never-smokers and 0.54 (95% CI: 0.38-0.76) for ever-smokers (p < .007 by metaregression). The pooled PFS HR for exon 19 deletion was 0.25 (95% CI: 0.19-0.31) and 0.44 for exon 21 substitution (95% CI: 0.34-0.57) (p < .001 by metaregression analysis). The pooled PFS HR was 0.33 (95% CI: 0.24-0.46) for Asians and 0.48 for non-Asians (95% CI: 0.28-0.84) (p = .261 by metaregression analysis).
Conclusion: EGFRm NSCLC patients derived significant PFS benefit from TKI over platinum-doublet chemotherapy as first-line treatment regardless of smoking status; however, PFS benefit is significantly better in never-smokers by metaregression analysis.
摘要
背景。来自几项 III 期随机试验的单变量分析似乎提示:通过无进展生存期 (PFS) 进行测量,与铂类双药化疗相比时,患有表皮生长因子受体突变 (EGFRm) 晚期非小细胞肺癌 (NSCLC) 的过去吸烟者似乎未从一线EGFR 酪氨酸激酶抑制剂 (TKI) 治疗中获益。
方法。使用随机效应模型,基于文献对通过对数转换汇总风险比 (HR) 所测量的 PFS 转归进行meta分析。获得了吸烟状态、年龄、性别、种族、EGFR 突变类型和 EGFR TKI 的汇总 HR。通过meta回归分析比较汇总的 HR。
结果。从 7 项前瞻性随机试验(WJTOG3405、NEJ002、EURTAC、OPTIMAL、LUX Lung-3、LUX Lung-6 和 ENSURE)分析的 1 649 名 EGFRm NSCLC 患者当中,83.7% 患者是亚裔,并且 30.0% 患者是过去吸烟者。相等百分数的过去吸烟者接受双药化疗 (30.2%) 或 EGFR TKI (30.0%)。对于从不吸烟者,PFS 的汇总 HR 是 0.29 [95% 置信区间( CI):0.21–0.39],而对于过去吸烟者,是 0.54(95% CI:0.38-0.76)(通过meta回归分析,p < 0.007)。对于外显子 19 缺失,PFS 的汇总 HR 是 0.25(95% CI:0.19-0.31),而对于外显子 21 置换,是 0.44(95% CI:0.34-0.57)(通过meta回归分析,p < 0.001)。对于亚裔,PFS 的汇总 HR 是 0.33(95% CI:0.24-0.46),而对于非亚裔是 0.48 (95% CI:0.28-0.84)(通过meta回归分析,p = 0.261)。
结论。EGFRm NSCLC 患者无论吸烟状态如何,从一线 TKI 治疗的 PFS 获益优于铂类双药化疗;然而,meta 回归分析显示,PFS 获益在从不吸烟者中明显更好。The Oncologist 2015; 20:307–315
Keywords: Afatinib; EGFR TKIs; EGFR mutant non-small cell lung cancer; Erlotinib; Gefitinib; Meta-analysis; Smoking status.
©AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121–128. - PubMed
-
- Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. - PubMed
-
- Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–742. - PubMed
-
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. - PubMed
-
- Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327–3334. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
