

Platelet rich clots are resistant to lysis by thrombolytic therapy in a rat model of embolic stroke
- PMID: 25657829
- PMCID: PMC4318170
- DOI: 10.1186/s13231-014-0014-y
Platelet rich clots are resistant to lysis by thrombolytic therapy in a rat model of embolic stroke
Abstract
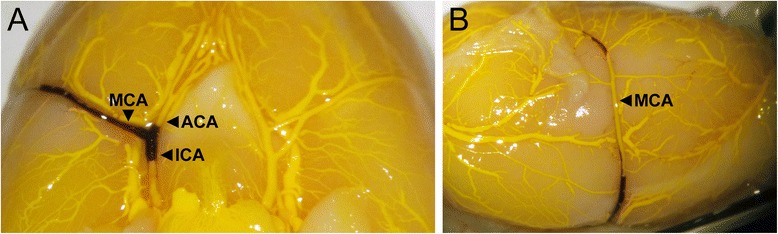
Background: Early recanalization of occluded vessels in stroke is closely associated with improved clinical outcome. Microbubble-enhanced sonothrombolysis is a promising therapy to improve recanalization rates and reduce the time to recanalization. Testing any thrombolytic therapy requires a model of thromboembolic stroke, but to date these models have been highly variable with regards to clot stability. Here, we developed a model of thromboembolic stroke in rats with site-specific delivery of platelet-rich clots (PRC) to the main stem of the middle cerebral artery (MCA). This model was used in a subsequent study to test microbubble-enhanced sonothrombolysis.
Methods: In Study 1 we investigated spontaneous recanalization rates of PRC in vivo over 4 hours and measured infarct volumes at 24 hours. In Study 2 we investigated tPA-mediated thrombolysis and microbubble-enhanced sonothrombolysis in this model.
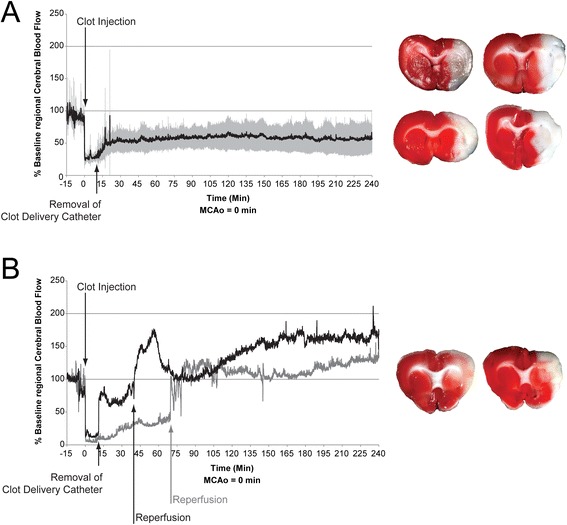
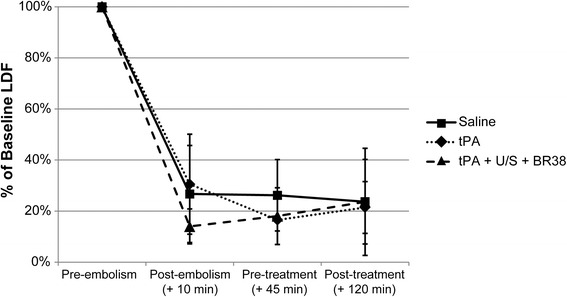
Results: Study 1 demonstrated stable occlusion out to 4 hours in 5 of 7 rats. Two rats spontaneously recanalized at 40 and 70 minutes post-embolism. Infarct volumes were not significantly different in recanalized rats, 43.93 ± 15.44% of the ischemic hemisphere, compared to 48.93 ± 3.9% in non-recanalized animals (p = 0.7). In Study 2, recanalization was not observed in any of the groups post-treatment.
Conclusions: Site specific delivery of platelet rich clots to the MCA origin resulted in high rates of MCA occlusion, low rates of spontaneous clot lysis and large infarction. These platelet rich clots were highly resistant to tPA with or without microbubble-enhanced sonothrombolysis. This resistance of platelet rich clots to enhanced thrombolysis may explain recanalization failures clinically and should be an impetus to better clot-type identification and alternative recanalization methods.
Keywords: Embolic Stroke; Microbubbles; Platelet Rich Clot; Rat; Sonothrombolysis; Thrombolysis; Ultrasound.
Figures
Similar articles
-
Microbubble-Mediated Sonothrombolysis Improves Outcome After Thrombotic Microembolism-Induced Acute Ischemic Stroke.Stroke. 2016 May;47(5):1344-53. doi: 10.1161/STROKEAHA.115.012056. Epub 2016 Apr 5. Stroke. 2016. PMID: 27048701
-
Microbubble administration accelerates clot lysis during continuous 2-MHz ultrasound monitoring in stroke patients treated with intravenous tissue plasminogen activator.Stroke. 2006 Feb;37(2):425-9. doi: 10.1161/01.STR.0000199064.94588.39. Epub 2005 Dec 22. Stroke. 2006. PMID: 16373632
-
Recanalization therapies for acute ischemic stroke.Semin Neurol. 1998;18(4):471-84. doi: 10.1055/s-2008-1040900. Semin Neurol. 1998. PMID: 9932618 Review.
-
Do bubble characteristics affect recanalization in stroke patients treated with microbubble-enhanced sonothrombolysis?Ultrasound Med Biol. 2008 Oct;34(10):1573-7. doi: 10.1016/j.ultrasmedbio.2008.02.011. Epub 2008 May 1. Ultrasound Med Biol. 2008. PMID: 18450360 Clinical Trial.
-
Is sonothrombolysis an effective stroke treatment?J Ultrasound Med. 2013 Jul;32(7):1117-23. doi: 10.7863/ultra.32.7.1117. J Ultrasound Med. 2013. PMID: 23804334 Review.
Cited by
-
PD-L1 Regulates Platelet Activation and Thrombosis via Caspase-3/GSDME Pathway.Front Pharmacol. 2022 Jun 15;13:921414. doi: 10.3389/fphar.2022.921414. eCollection 2022. Front Pharmacol. 2022. PMID: 35784685 Free PMC article.
-
Sonothrombolysis for Ischemic Stroke.J Cardiovasc Dev Dis. 2024 Feb 22;11(3):75. doi: 10.3390/jcdd11030075. J Cardiovasc Dev Dis. 2024. PMID: 38535098 Free PMC article. Review.
-
Microbubbles combined with ultrasound therapy in ischemic stroke: A systematic review of in-vivo preclinical studies.PLoS One. 2018 Feb 8;13(2):e0191788. doi: 10.1371/journal.pone.0191788. eCollection 2018. PLoS One. 2018. PMID: 29420546 Free PMC article.
-
Extracellular DNA-A Danger Signal Triggering Immunothrombosis.Front Immunol. 2020 Oct 7;11:568513. doi: 10.3389/fimmu.2020.568513. eCollection 2020. Front Immunol. 2020. PMID: 33117353 Free PMC article. Review.
-
"Going with the flow" in modeling fibrinolysis.Front Cardiovasc Med. 2022 Dec 2;9:1054541. doi: 10.3389/fcvm.2022.1054541. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36531720 Free PMC article. Review.
References
-
- National Stroke Foundation . National Stroke Audit - Acute Services Clinical Audit Report 2011. Melbourne, Australia: National Stroke Foundation; 2011.
-
- Alexandrov AV, Demchuk AM, Felberg RA, Christou I, Barber PA, Burgin WS, et al. High rate of complete recanalization and dramatic clinical recovery during tPA infusion when continuously monitored with 2-MHz transcranial doppler monitoring. Stroke. 2000;31:610–614. doi: 10.1161/01.STR.31.3.610. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
