

Obesity increases airway hyperresponsiveness via the TNF-α pathway and treating obesity induces recovery
- PMID: 25658739
- PMCID: PMC4344461
- DOI: 10.1371/journal.pone.0116540
Obesity increases airway hyperresponsiveness via the TNF-α pathway and treating obesity induces recovery
Abstract
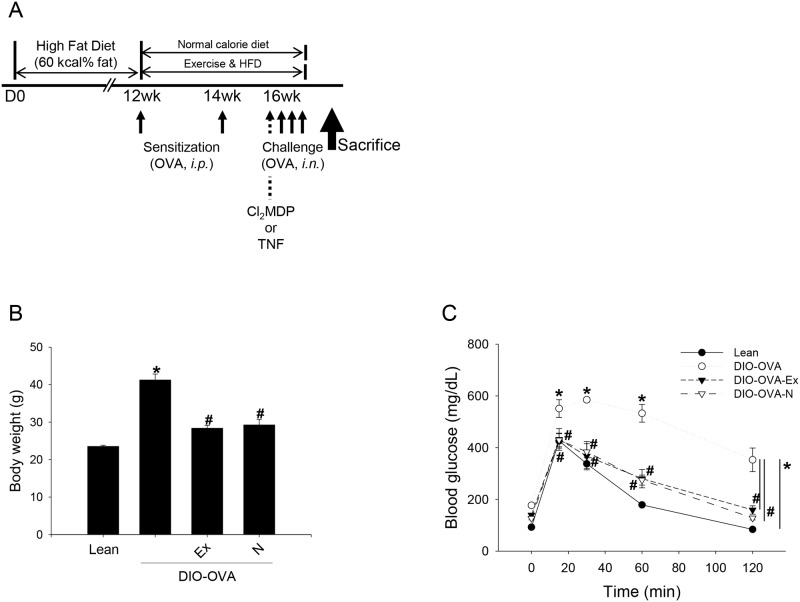
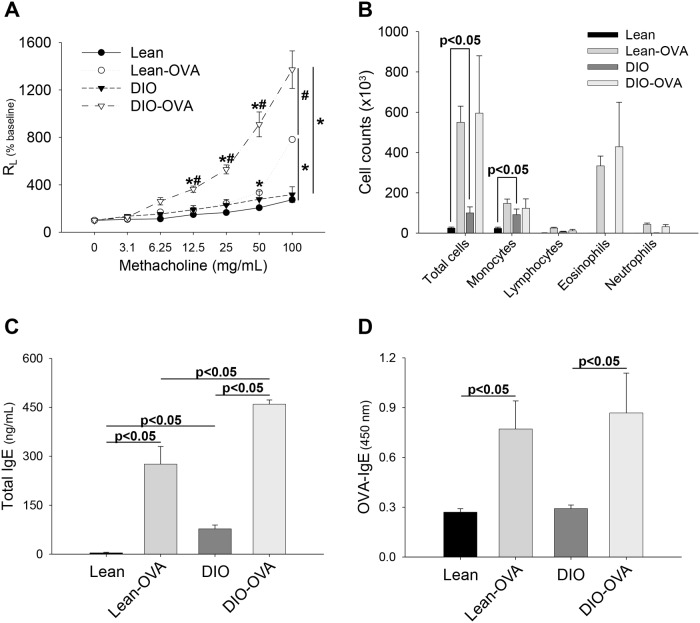
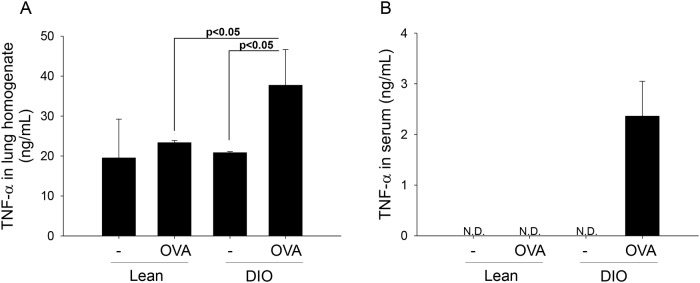
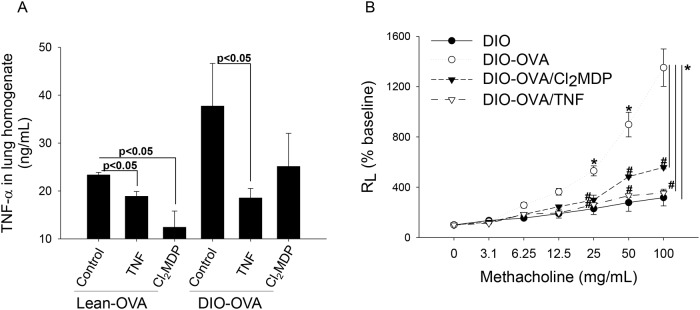
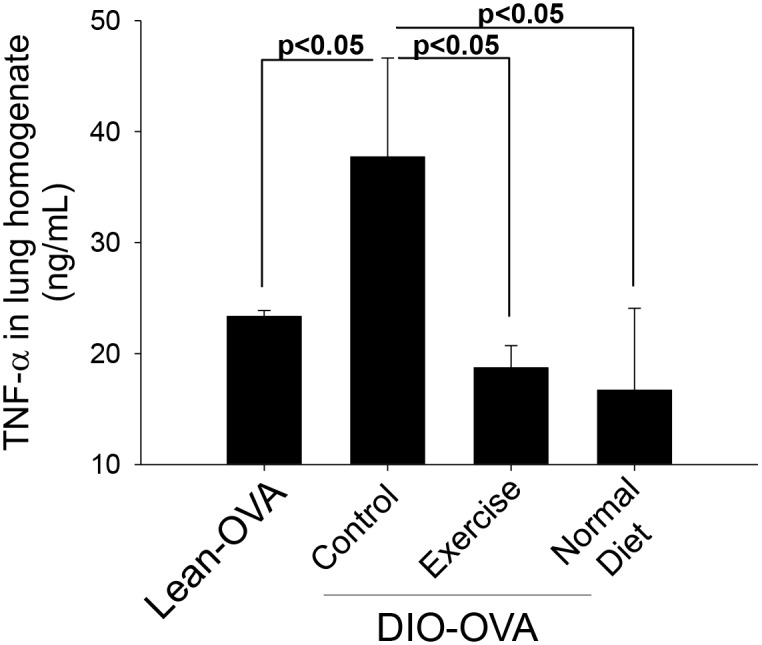
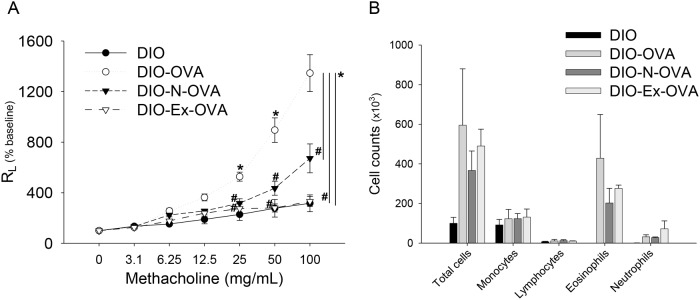
Obesity is a known risk factor for allergic asthma. It has been recognized as a key player in the pathogenesis of several inflammatory disorders via activation of macrophages, which is also vital to the development of allergic asthma. We investigated the mechanism of obesity-related asthma and whether treating obesity through exercise or diet ameliorates the severity of asthma in the obesity-related asthma model. We generated diet-induced obesity (DIO) in C57BL/6 mice by high-fat-feeding and ovalbumin-induced asthma (lean-OVA or DIO-OVA). The DIO-OVA mice were then treated with tumor necrosis factor (TNF)-α neutralizing antibody as a TNF-α blockade or a Cl2MDP-containing liposome to induce an alveolar macrophage deficiency. To treat obesity, the DIO-OVA mice were under dietary restrictions or exercised. The pathophysiological and immunological responses were analyzed. Airway hyperresponsiveness (AHR), serum IgE and TNF-α levels in the lung tissue increased in the DIO-OVA mice compared to the lean-OVA mice. Both the TNF-α blockade and depletion of alveolar macrophages in the DIO-OVA mice decreased AHR compared to the DIO-OVA mice. Treating obesity by exercise or through dietary means also reduced pulmonary TNF-α levels and AHR in the DIO-OVA mice. These results suggest that restoring normal body weight is an appropriate strategy for reducing TNF-α levels, and controlling inflammation may help improve asthma severity and control in obesity-related asthma.
Conflict of interest statement
Figures
References
-
- Organization WH (2006) Obesity and overweight (WHO Fact Sheet No. 311) WHO Media centre 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
