

Challenges in EGFRvIII detection in head and neck squamous cell carcinoma
- PMID: 25658924
- PMCID: PMC4320077
- DOI: 10.1371/journal.pone.0117781
Challenges in EGFRvIII detection in head and neck squamous cell carcinoma
Abstract
Objective: Head and neck squamous cell carcinoma (HNSCC) accounts for more than 5% of all cancers worldwide. The mortality rate of HNSCC has remained unchanged (approximately 50%) over the last few decades. Ubiquitous overexpression of wild type EGFR in many solid tumors has led to the development of EGFR targeted therapies. EGFR can be constitutively activated via several mechanisms including the truncated, EGFR variant III isoform (EGFRvIII). EGFRvIII lacks exons 2-7 and has been reported to be present in up to 20-40% of HNSCC. EGFRvIII has been shown to contribute to cetuximab resistance. The mechanisms leading to EGFRvIII expression in HNSCC are unknown. The present investigation was undertaken to determine the etiology of EGFRvIII in HNSCC.
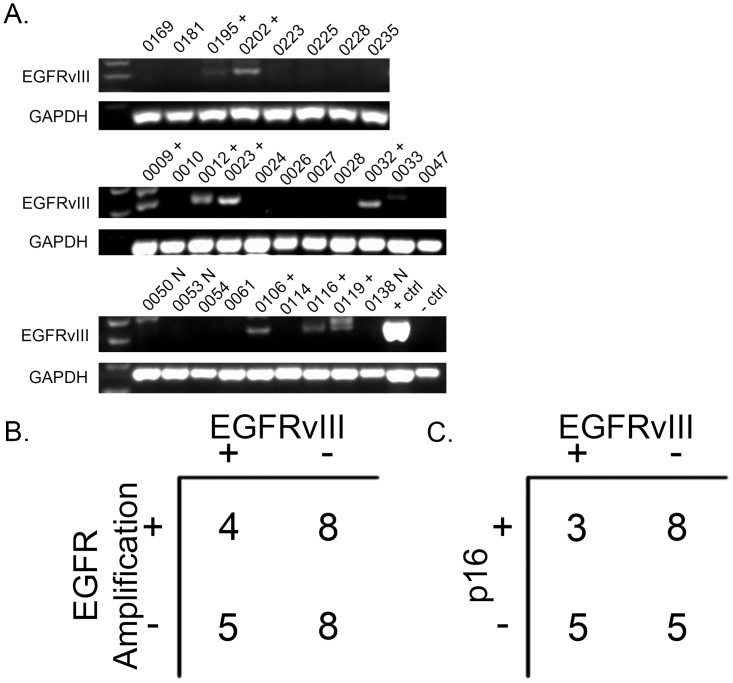
Materials and methods: Fixed HNSCC and glioma tissues were analyzed by fluorescence in situ hybridization for EGFR amplification. DNA and RNA from fresh frozen specimens were used to determine the presence of EGFRvIII transcripts and the mechanisms of expression via PCR, RT-PCR and RNA sequencing.
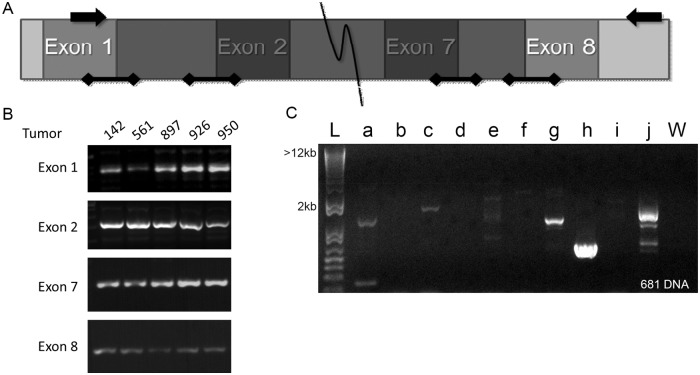
Results: Unlike glioma, EGFRvIII expression in HNSCC did not correlate with EGFR amplification. We found evidence of genomic deletion of the exon 2-7 in 6 of 7 HNSCC cases examined, however, the presence of genomic deletion did not always result in mRNA expression of EGFRvIII. RNA sequencing with automated alignment did not identify EGFRvIII due to microhomology between intron 1 and exon 8. RNA sequencing analyzed by manual alignment methods did not correlate well with RT-PCR and PCR findings.
Conclusion: These findings suggest that genomic deletion as well as additional regulatory mechanisms may contribute to EGFRvIII expression in HNSCC. Further, large scale automated alignment of sequencing are unlikely to identify EGFRvIII and an assay specifically designed to detect EGFRvIII may be necessary to detect this altered form of EGFR in HNSCC tumors.
Conflict of interest statement
Figures
Similar articles
-
Epidermal growth factor receptor variant III in head and neck squamous cell carcinoma is not relevant for targeted therapy and irradiation.Oncotarget. 2017 May 16;8(20):32668-32682. doi: 10.18632/oncotarget.15949. Oncotarget. 2017. PMID: 28427242 Free PMC article.
-
Tumor epidermal growth factor receptor and EGFR PY1068 are independent prognostic indicators for head and neck squamous cell carcinoma.Clin Cancer Res. 2012 Apr 15;18(8):2278-89. doi: 10.1158/1078-0432.CCR-11-1593. Epub 2012 Feb 20. Clin Cancer Res. 2012. PMID: 22351687 Free PMC article.
-
Mutant epidermal growth factor receptor (EGFRvIII) contributes to head and neck cancer growth and resistance to EGFR targeting.Clin Cancer Res. 2006 Sep 1;12(17):5064-73. doi: 10.1158/1078-0432.CCR-06-0913. Clin Cancer Res. 2006. PMID: 16951222
-
PET Imaging in Head and Neck Cancer Patients to Monitor Treatment Response: A Future Role for EGFR-Targeted Imaging.Clin Cancer Res. 2015 Aug 15;21(16):3602-9. doi: 10.1158/1078-0432.CCR-15-0348. Epub 2015 Apr 30. Clin Cancer Res. 2015. PMID: 25931452 Review.
-
Epidermal growth factor receptor (EGFR) and squamous cell carcinoma of the skin: molecular bases for EGFR-targeted therapy.Pathol Res Pract. 2011 Jun 15;207(6):337-42. doi: 10.1016/j.prp.2011.03.002. Epub 2011 Apr 29. Pathol Res Pract. 2011. PMID: 21531084 Review.
Cited by
-
The CRISPR-Cas revolution in head and neck cancer: a new era of targeted therapy.Funct Integr Genomics. 2025 May 30;25(1):113. doi: 10.1007/s10142-025-01612-2. Funct Integr Genomics. 2025. PMID: 40445465 Review.
-
Visualizing Genetic Variants, Short Targets, and Point Mutations in the Morphological Tissue Context with an RNA In Situ Hybridization Assay.J Vis Exp. 2018 Aug 14;(138):58097. doi: 10.3791/58097. J Vis Exp. 2018. PMID: 30176002 Free PMC article.
-
Major Molecular Signaling Pathways in Oral Cancer Associated With Therapeutic Resistance.Front Oral Health. 2021 Jan 25;1:603160. doi: 10.3389/froh.2020.603160. eCollection 2020. Front Oral Health. 2021. PMID: 35047986 Free PMC article. Review.
-
Head and neck cancer: the role of anti-EGFR agents in the era of immunotherapy.Ther Adv Med Oncol. 2021 Mar 9;13:1758835920949418. doi: 10.1177/1758835920949418. eCollection 2021. Ther Adv Med Oncol. 2021. PMID: 33767760 Free PMC article. Review.
-
Co-expression of HER2/EGFRvIII/CD44 and Claudin 18.2/CD109 as Novel Prognostic Indicators in Stomach Adenocarcinoma.World J Oncol. 2025 Jun;16(3):254-268. doi: 10.14740/wjon2552. Epub 2025 Apr 4. World J Oncol. 2025. PMID: 40556965 Free PMC article.
References
-
- Parkin DM, Pisani P, Ferlay J (1999) Global cancer statistics. CA Cancer J Clin 49: 33–64, 31 - PubMed
-
- Grandis JR, Tweardy DJ (1993) Elevated levels of transforming growth factor alpha and epidermal growth factor receptor messenger RNA are early markers of carcinogenesis in head and neck cancer. Cancer Res 53: 3579–3584. - PubMed
-
- Grandis JR, Melhem MF, Barnes EL, Tweardy DJ (1996) Quantitative immunohistochemical analysis of transforming growth factor- alpha and epidermal growth factor receptor in patients with squamous cell carcinoma of the head and neck. Cancer 78: 1284–1292. - PubMed
-
- Arteaga CL (2002) Overview of epidermal growth factor receptor biology and its role as a therapeutic target in human neoplasia. Semin Oncol 29: 3–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
