

Clinical Aspects of Adult Tuberculosis
- PMID: 25659379
- PMCID: PMC4691808
- DOI: 10.1101/cshperspect.a017848
Clinical Aspects of Adult Tuberculosis
Abstract
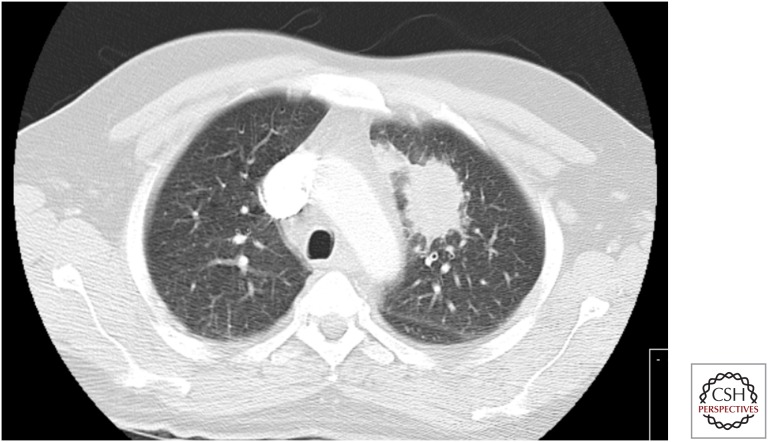
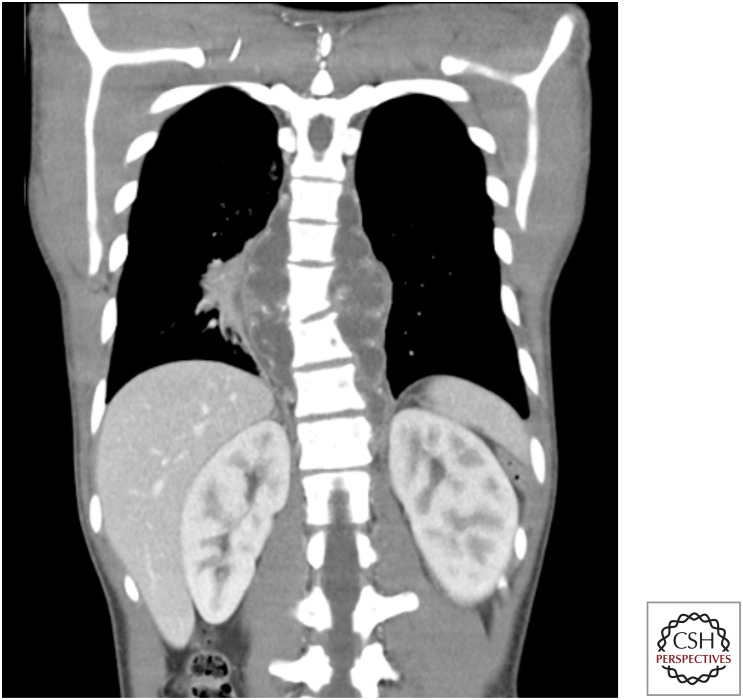
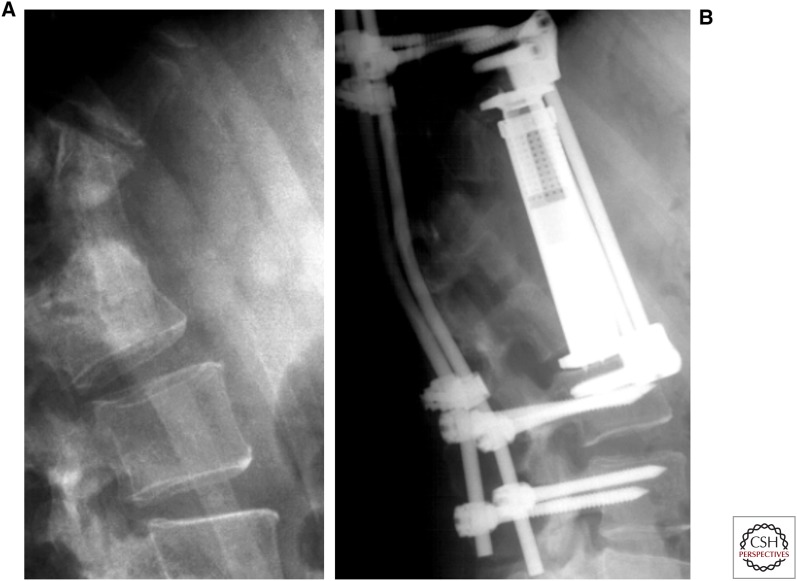
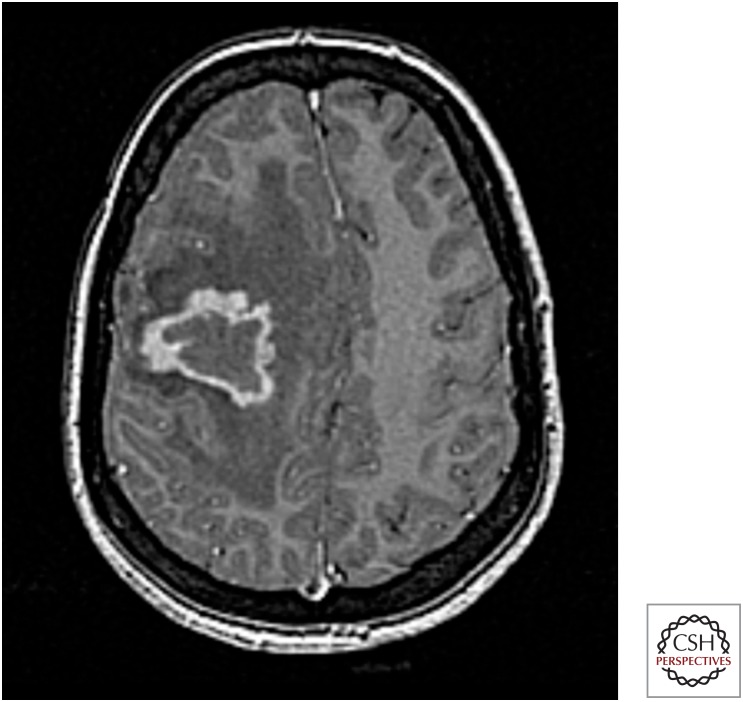
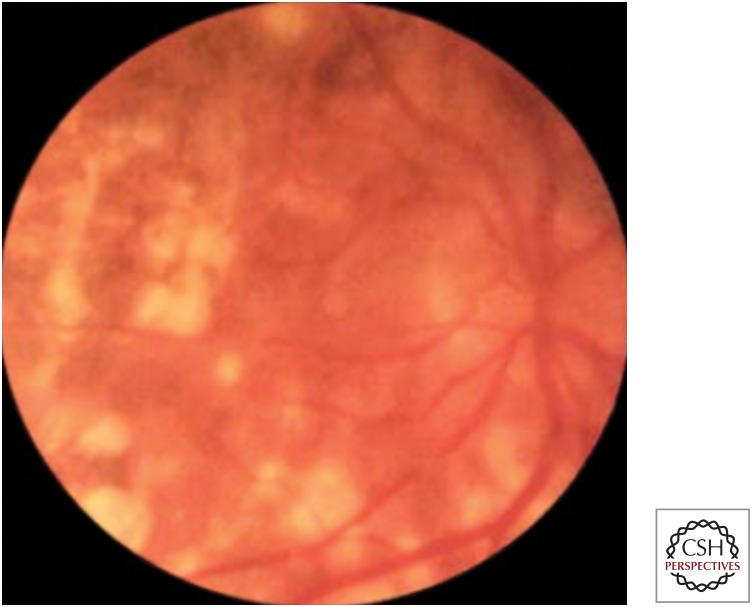
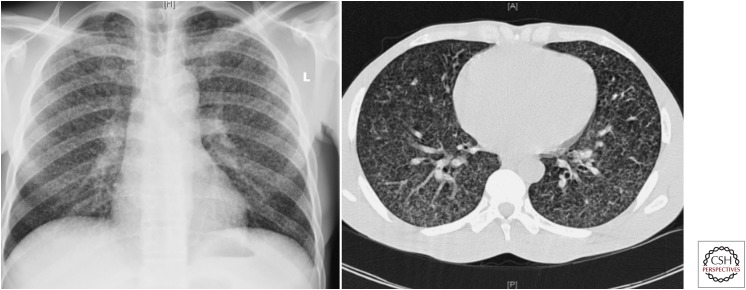
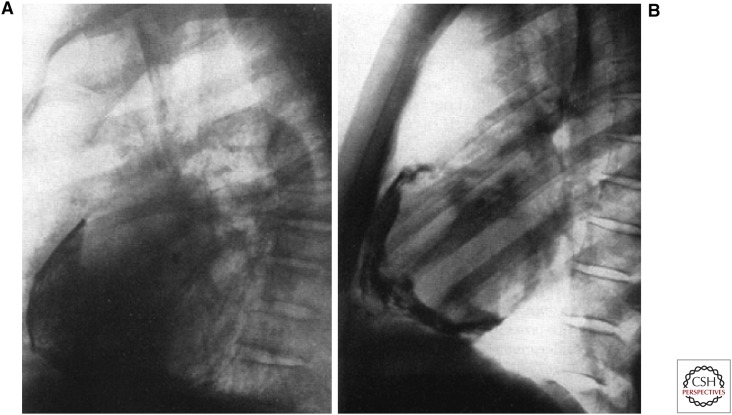
Tuberculosis (TB) in adults can present in a large number of ways. The lung is the predominant site of TB. Primary pulmonary TB should be distinguished from postprimary pulmonary TB, which is the most frequent TB manifestation in adults (70%-80% cases). Cough is common, although the chest radiograph often raises suspicion of disease. Sputum sampling is a key step in the diagnosis of TB, and invasive procedures such as bronchoscopy may be necessary to achieve adequate samples for diagnosis. Extrapulmonary involvement, which may present many years after exposure, occurs in a variable proportion of cases (20%-45%). This reflects the country of origin of patients and also the frequency of associated human immunodeficiency virus (HIV) coinfection. In the latter case, the presentation of TB is often nonspecific, and care needs to be taken to not miss the diagnosis. Anti-TB therapy should be given in line with proven (or assumed) drug resistance. In extrapulmonary TB, adjunctive therapeutic measures may be indicated; although in all cases, support is often required to ensure that people are able to complete treatment with minimal adverse events and maximal adherence to the prescribed regimen, and so reduce risk of future disease for themselves and others.
Copyright © 2016 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures


















References
-
- Aït-Khaled N, Alarcón E, Armengol R, Bissell K, Boillot F, Caminero JA, Chiang C-Y, Clevenbergh P, Dlodlo R, Enarson DA, et al. 2010. Management of tuberculosis: A guide to the essentials of good practice. Paris, France, International Union Against Tuberculosis and Lung Disease (The Union) http://www.theunion.org/what-we-do/publications/technical/english/pub_or...
-
- Almadi MA, Ghosh S, Aljebreen AM. 2009. Differentiating intestinal tuberculosis from Crohn’s disease: A diagnostic challenge. Am J Gastroenterol 104: 1003–1012. - PubMed
-
- Anderson C, White J, Abubakar I, Lipman M, Tamne S, Anderson SR, deKoningh J, Dart S. 2014. Raising standards in UK TB control: Introducing cohort review. Thorax 69: 187–189. - PubMed
-
- Bernaerts A, Vanhoenacker FM, Parizel PM, Van Goethem JW, Van Altena R, Laridon A, De Roeck J, Coeman V, De Schepper AM. 2003. Tuberculosis of the central nervous system: Overview of neuroradiological findings. Eur Radiol 13: 1876–1890. - PubMed
-
- Bhat VK, Latha P, Upadhya D, Hegde J. 2009. Clinicopathological review of tubercular laryngitis in 32 cases of pulmonary Kochs. Am J Otolaryngol 30: 327–330. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical