

Lung cancer diagnosis and staging with endobronchial ultrasound-guided transbronchial needle aspiration compared with conventional approaches: an open-label, pragmatic, randomised controlled trial
- PMID: 25660225
- PMCID: PMC4648022
- DOI: 10.1016/S2213-2600(15)00029-6
Lung cancer diagnosis and staging with endobronchial ultrasound-guided transbronchial needle aspiration compared with conventional approaches: an open-label, pragmatic, randomised controlled trial
Abstract
Background: The diagnosis and staging of lung cancer is an important process that identifies treatment options and guides disease prognosis. We aimed to assess endobronchial ultrasound-guided transbronchial needle aspiration as an initial investigation technique for patients with suspected lung cancer.
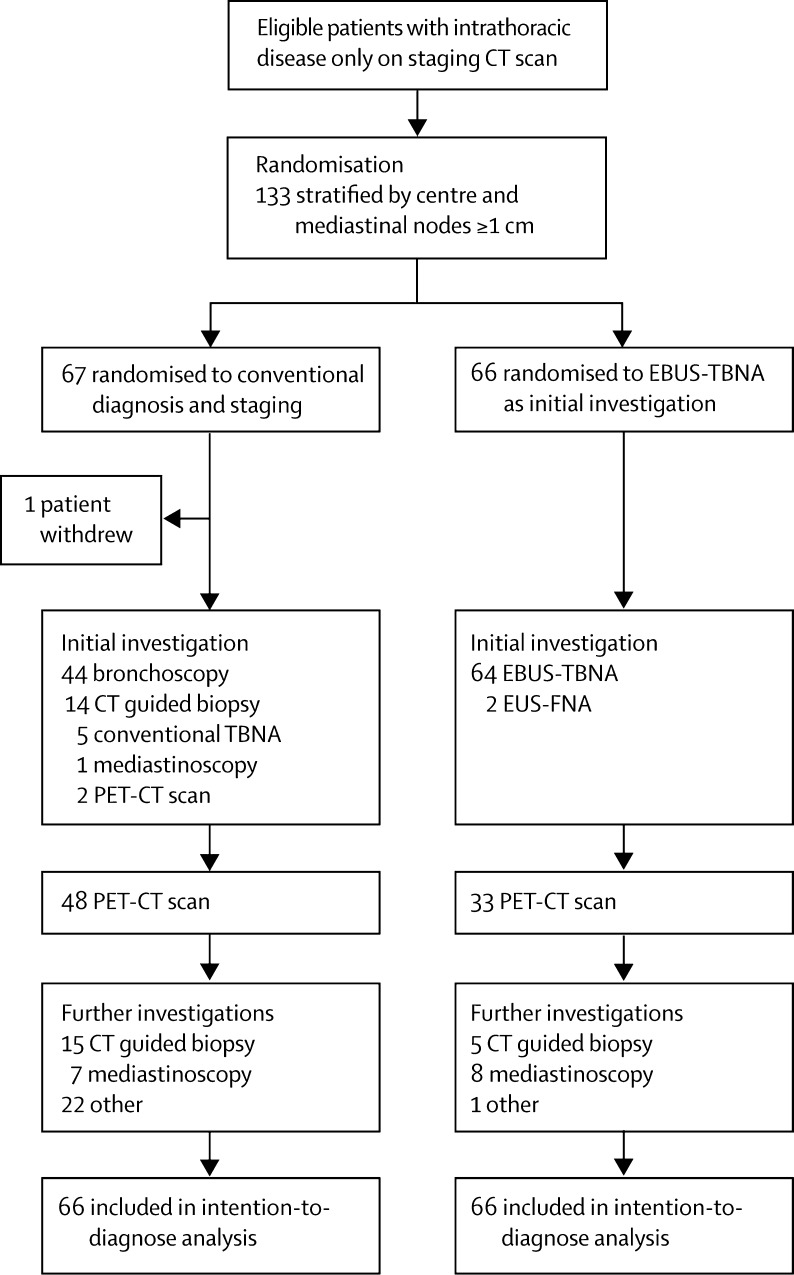
Methods: In this open-label, multicentre, pragmatic, randomised controlled trial, we recruited patients who had undergone a CT scan and had suspected stage I to IIIA lung cancer, from six UK centres and randomly assigned them to either endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) or conventional diagnosis and staging (CDS), for further investigation and staging. If a target node could not be accessed by EBUS-TBNA, then endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) was allowed as an alternative procedure. Randomisation was stratified according to the presence of mediastinal lymph nodes measuring 1 cm or more in the short axis and by recruiting centre. We used a telephone randomisation method with permuted blocks of four generated by a computer. Because of the nature of the intervention, masking of participants and consenting investigators was not possible. The primary endpoint was the time-to-treatment decision after completion of the diagnostic and staging investigations and analysis was by intention-to-diagnose. This trial is registered with ClinicalTrials.gov, number NCT00652769.
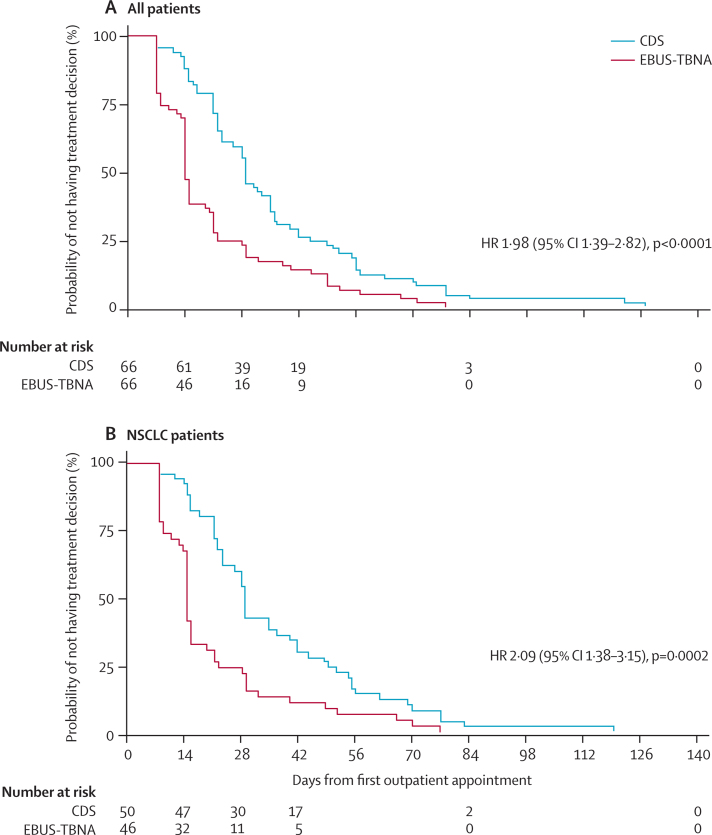
Findings: Between June 10, 2008, and July 4, 2011, we randomly allocated 133 patients to treatment: 66 to EBUS-TBNA and 67 to CDS (one later withdrew consent). Two patients from the EBUS-TBNA group underwent EUS-FNA. The median time to treatment decision was shorter with EBUS-TBNA (14 days; 95% CI 14-15) than with CDS (29 days; 23-35) resulting in a hazard ratio of 1·98, (1·39-2·82, p<0·0001). One patient in each group had a pneumothorax from a CT-guided biopsy sample; the patient from the CDS group needed intercostal drainage and was admitted to hospital.
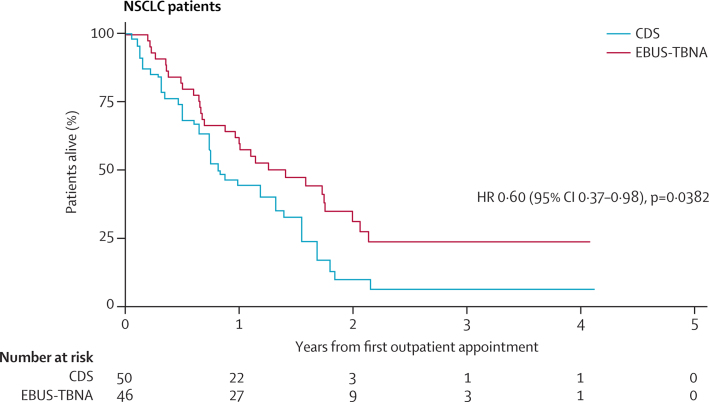
Interpretation: Transbronchial needle aspiration guided by endobronchial ultrasound should be considered as the initial investigation for patients with suspected lung cancer, because it reduces the time to treatment decision compared with conventional diagnosis and staging techniques.
Funding: UK Medical Research Council.
Copyright © 2015 Navani et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Lung cancer staging: a true story.Lancet Respir Med. 2015 Apr;3(4):258-9. doi: 10.1016/S2213-2600(15)00030-2. Epub 2015 Feb 4. Lancet Respir Med. 2015. PMID: 25660224 No abstract available.
References
-
- Jemal A, Bray F, Center MM. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- NICE Lung cancer guidelines. 2011. http://guidance.nice.org.uk/cg121 (accessed Jan 22, 2015).
-
- Ramnath N, Dilling TJ, Harris LJ. Treatment of non-small cell lung cancer-stage IIIA: treatment of stage III non-small cell lung cancer: diagnosis and management of lung cancer, 3rd edn. American college of chest physicians evidence-based clinical practice guidelines. Chest. 2013;143:e314S–e340S. - PubMed
-
- National Lung Cancer Audit Report, 2013. http://www.hscic.gov.uk/catalogue/PUB12719/clin-audi-supp-prog-lung-nlca... (accessed Jan 22, 2015).
-
- Silvestri GA, Gonzalez AV, Jantz MA. Methods for staging non-small cell lung cancer: diagnosis and management of lung cancer, 3rd edn. American college of chest physicians evidence-based clinical practice guidelines. Chest. 2013;143:e211S–e250S. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
