

The risk paradox: use of elective cholecystectomy in older patients is independent of their risk of developing complications
- PMID: 25660731
- PMCID: PMC4372464
- DOI: 10.1016/j.jamcollsurg.2014.12.012
The risk paradox: use of elective cholecystectomy in older patients is independent of their risk of developing complications
Abstract
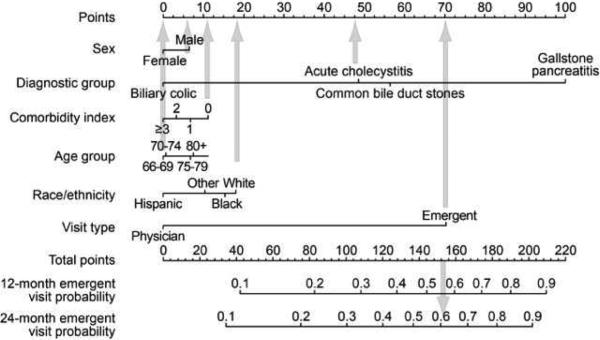
Background: We recently developed and validated a prognostic model that accurately predicts the 2-year risk of emergent gallstone-related hospitalization in older patients presenting with symptomatic gallstones.
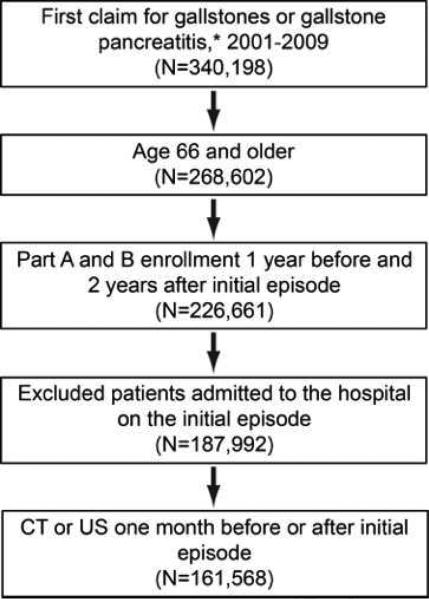
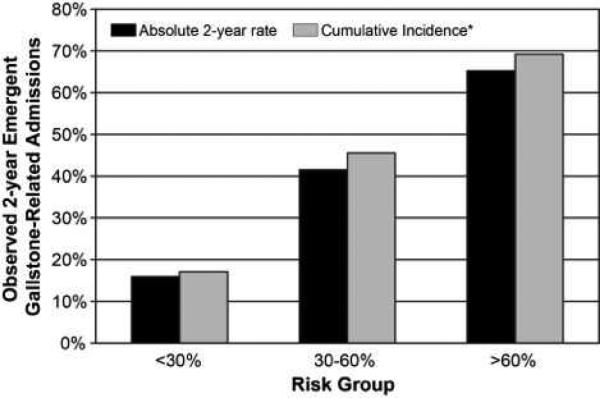
Study design: We used 100% Texas Medicare data (2000 to 2011) to identify patients aged 66 years and older with an initial episode of symptomatic gallstones not requiring emergency hospitalization. At presentation, we calculated each patient's risk of 2-year gallstone-related emergent hospitalization using the previously validated model. Patients were placed into the following risk groups based on model estimates: <30%, 30% to <60%, and ≥ 60%. Within each risk group, we calculated the percent of elective cholecystectomies (≤ 2.5 months from initial episode) performed.
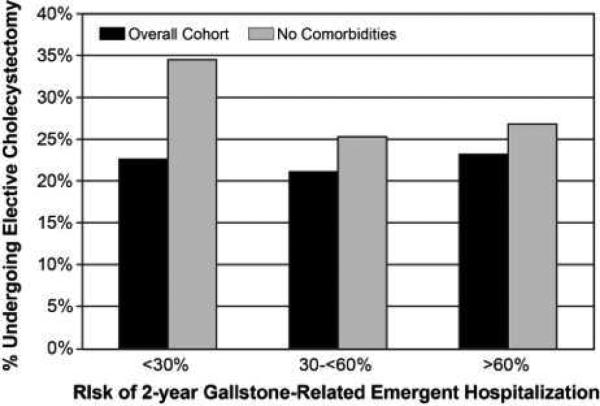
Results: In all, 161,568 patients had an episode of symptomatic gallstones. Mean age was 76.5 ± 7.3 years and 59.9% were female. The 2-year risk of gallstone-related hospitalizations increased from 15.9% to 41.5% to 65.2% across risk groups. For the overall cohort, 22.3% in the low-risk group, 20.9% in the moderate-risk group, and 23.2% in the high-risk group underwent elective cholecystectomy in the 2.5 months after the initial symptomatic episode. In patients with no comorbidities, elective cholecystectomy rates decreased from 34.2% in the low-risk group to 26.7% in the high-risk group. Of patients who did not undergo cholecystectomy, only 9.5% were seen by a surgeon in the 2.5 months after the initial episode.
Conclusions: The risk of recurrent acute biliary symptoms requiring hospitalization has no influence, or even a paradoxical negative influence, on the decision to perform elective cholecystectomy after an initial symptomatic episode. Translation of the risk prediction model into clinical practice can better align treatment with risk and improve outcomes in older patients with symptomatic gallstones.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2015 Apr;220(4):690-2. doi: 10.1016/j.jamcollsurg.2015.01.042. J Am Coll Surg. 2015. PMID: 25797755 No abstract available.
References
-
- Hendrickson M, Naparst TR. Abdominal surgical emergencies in the elderly. Emerg Med Clin North Am. 2003;21:937–969. - PubMed
-
- Bugliosi TF, Meloy TD, Vukov LF. Acute abdominal pain in the elderly. Annals of emergency medicine. 1990;19(12):1383–1386. - PubMed
-
- Attili AF, De Santis A, Capri R, Repice AM, Maselli S. The natural history of gallstones: the GREPCO experience. The GREPCO Group. Hepatology. 1995;21(3):655–660. - PubMed
-
- Festi D, Reggiani ML, Attili AF, et al. Natural history of gallstone disease: Expectant management or active treatment? Results from a population-based cohort study. Journal of gastroenterology and hepatology. 2010;25(4):719–724. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
