

Surgical embolectomy for acute massive pulmonary embolism
- PMID: 25664045
- PMCID: PMC4307492
Surgical embolectomy for acute massive pulmonary embolism
Abstract
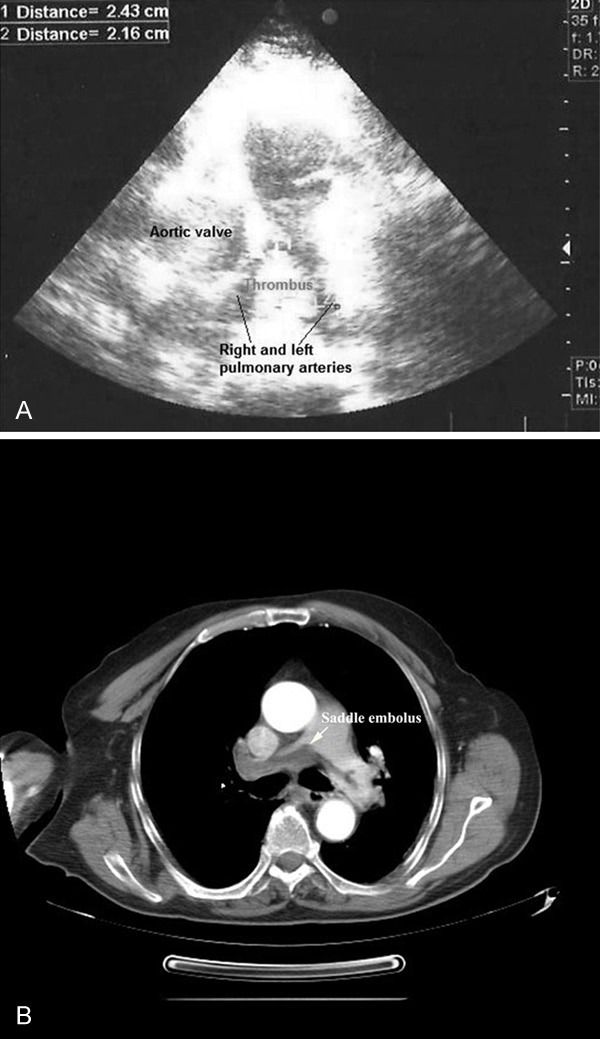
Objective: Acute massive pulmonary embolism (PE) is associated with significant mortality rate despite diagnostic and therapeutic advances. The aim of this study was to analyze our clinical outcomes of patients with acute massive PE who underwent emergency surgical pulmonary embolectomy.
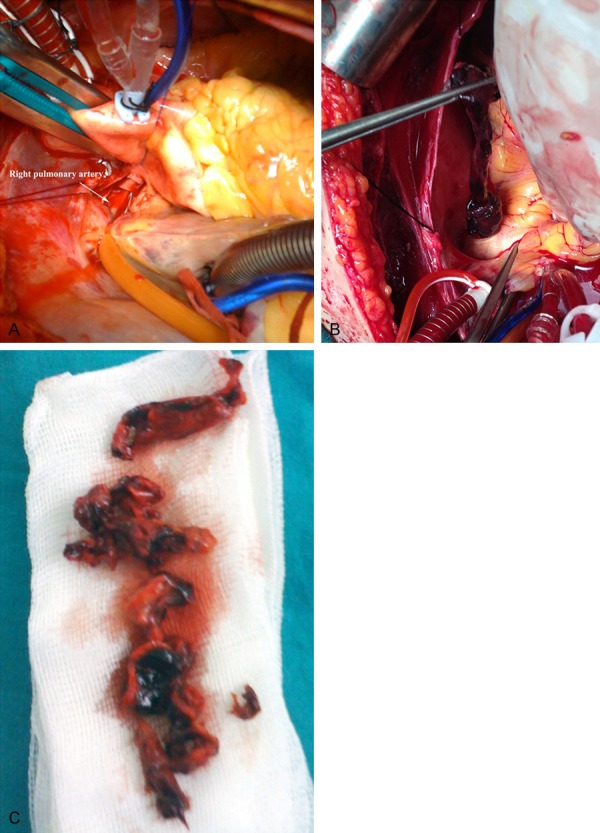
Methods: This retrospective study included 13 consecutive patients undergoing emergency surgical pulmonary embolectomy for acute massive PE at our institution from March 2000 to November 2013. The medical records of all patients were reviewed for demograhic and preoperative data and postoperative outcomes. All patients presented with cardiogenic shock with severe right ventricular dysfunction confirmed by echocardiography, where 4 (30.8%) of the patients experienced cardiac arrest requiring cardiopulmonary resuscitation before surgery.
Results: The mean age of patients was 61.8 ± 14 years (range, 38 to 82 years) with 8 (61.5%) males. The most common risk factors for PE was the history of prior deep venous thrombosis (n = 9, 69.2%). There were 3 (23.1%) in-hospital deaths including operative mortality of 7.7% (n = 1). Ten (76.9%) patients survived and were discharged from the hospital. The mean follow-up was 25 months; follow-up was 100% complete in surviving patients. There was one case (7.7%) of late death 12 months after surgery due to renal carcinoma. Postoperative echocardiographic pressure measurements demonstrated a significant reduction (P < 0.001). At final follow-up, all patients were in New York Heart Association class I and no readmission for a recurrent of PE was observed.
Conclusion: Surgical pulmonary embolectomy is a reasonable option and could be performed with acceptable results, if it is performed early in patients with acute massive PE who have not reached the profound cardiogenic shock or cardiac arrest.
Keywords: Acute massive pulmonary embolism; cardiopulmonary bypass; emergency operation; surgical embolectomy; thrombus.
Figures
References
-
- Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Massive pulmonary embolism. Circulation. 2006;113:577–582. - PubMed
-
- Goldhaber SZ, Elliott CG. Acute pulmonary embolism, I: epidemiology, pathophysiology, and diagnosis. Circulation. 2003;108:2726–2729. - PubMed
-
- Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER) Lancet. 1999;353:1386–1389. - PubMed
-
- Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galie N, Pruszczyk P, Bengel F, Brady AJ, Ferreira D, Janssens U, Klepetko W, Mayer E, Remy-Jandin M, Bassand JP ESC Committee for Practice Guidelines (CPG) Guidelines on the diagnosis and management of acute pulmonary embolism: the task force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC) Eur Heart J. 2008;18:2276–2315. - PubMed
-
- Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, Jenkins JS, Kline JA, Michaels AD, Thistlethwaite P, Vedantham S, White RJ, Zierler BK American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788–830. - PubMed
LinkOut - more resources
Full Text Sources