

The evolving molecular genetics of low-grade glioma
- PMID: 25664944
- PMCID: PMC4667550
- DOI: 10.1097/PAP.0000000000000049
The evolving molecular genetics of low-grade glioma
Erratum in
- Adv Anat Pathol. 2015 May;22(3):226
Abstract
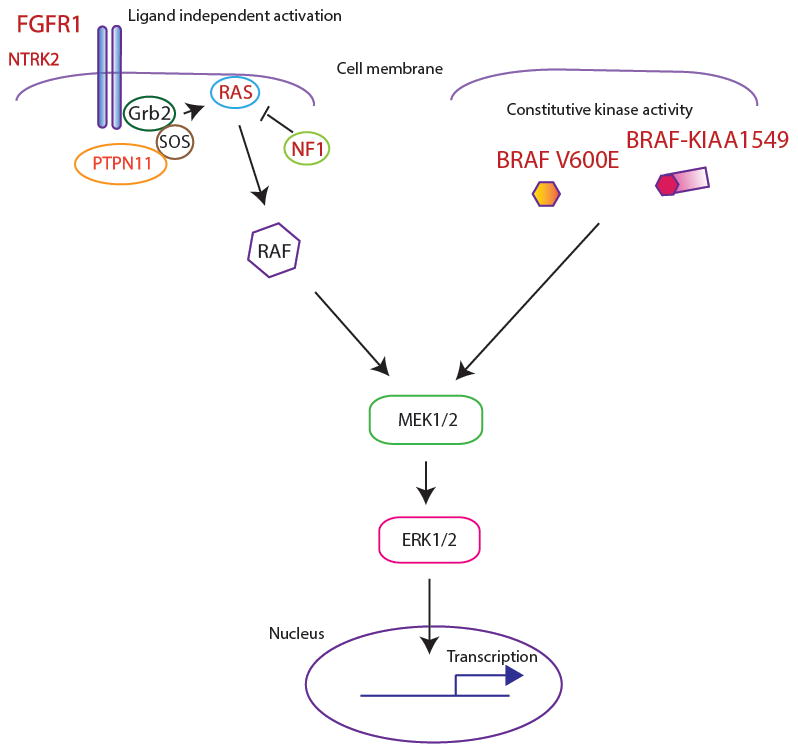
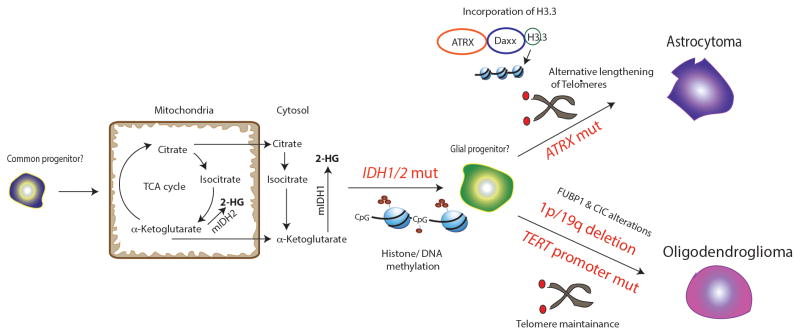
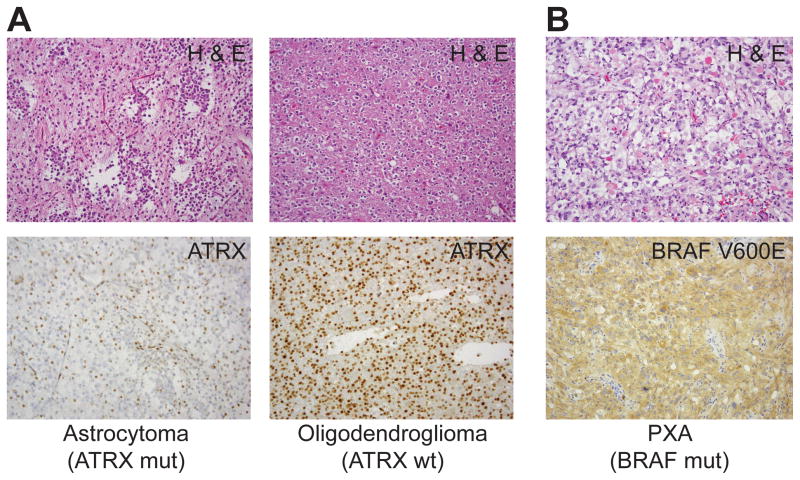
Low-grade gliomas (LGG) constitute grades I and II tumors of astrocytic and grade II tumors of oligodendroglial lineage. Although these tumors are typically slow growing, they may be associated with significant morbidity and mortality because of recurrence and malignant progression, even in the setting of optimal resection. LGG in pediatric and adult age groups are currently classified by morphologic criteria. Recent years have heralded a molecular revolution in understanding brain tumors, including LGG. Next-generation sequencing has definitively demonstrated that pediatric and adult LGG fundamentally differ in their underlying molecular characteristics, despite being histologically similar. Pediatric LGG show alterations in FGFR1 and BRAF in pilocytic astrocytomas and FGFR1 alterations in diffuse astrocytomas, each converging on the mitogen-activated protein kinase signaling pathway. Adult LGG are characterized by IDH1/2 mutations and ATRX mutations in astrocytic tumors and IDH1/2 mutations and 1p/19q codeletions in oligodendroglial tumors. TERT promoter mutations are also noted in LGG and are mainly associated with oligodendrogliomas. These findings have considerably refined approaches to classifying these tumors. Moreover, many of the molecular alterations identified in LGG directly impact on prognosis, tumor biology, and the development of novel therapies.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- Schwartzentruber J, Korshunov A, Liu XY, et al. Driver mutations in histone H3. 3 and chromatin remodelling genes in paediatric glioblastoma. Nature. 2012;482:226–231. - PubMed
-
- Bar EE, Lin A, Tihan T, et al. Frequent gains at chromosome 7q34 involving BRAF in pilocytic astrocytoma. Journal of neuropathology and experimental neurology. 2008;67:878–887. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
