

Current but not past smoking increases the risk of cardiac events: insights from coronary computed tomographic angiography
- PMID: 25666322
- PMCID: PMC4416139
- DOI: 10.1093/eurheartj/ehv013
Current but not past smoking increases the risk of cardiac events: insights from coronary computed tomographic angiography
Abstract
Aims: We evaluated coronary artery disease (CAD) extent, severity, and major adverse cardiac events (MACEs) in never, past, and current smokers undergoing coronary CT angiography (CCTA).
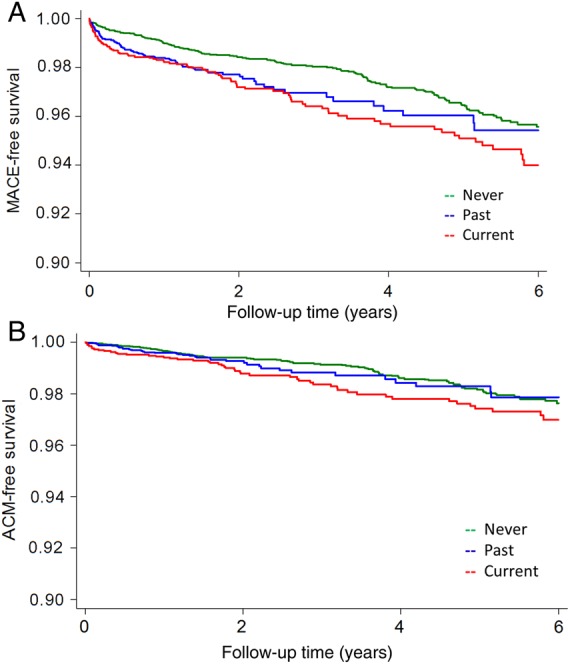
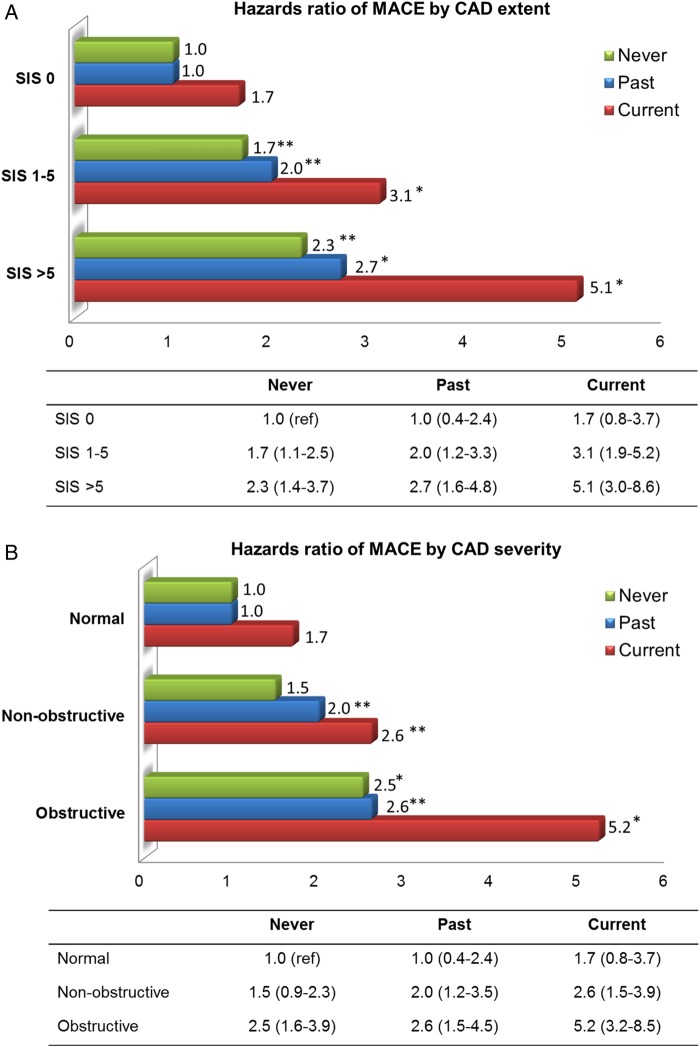
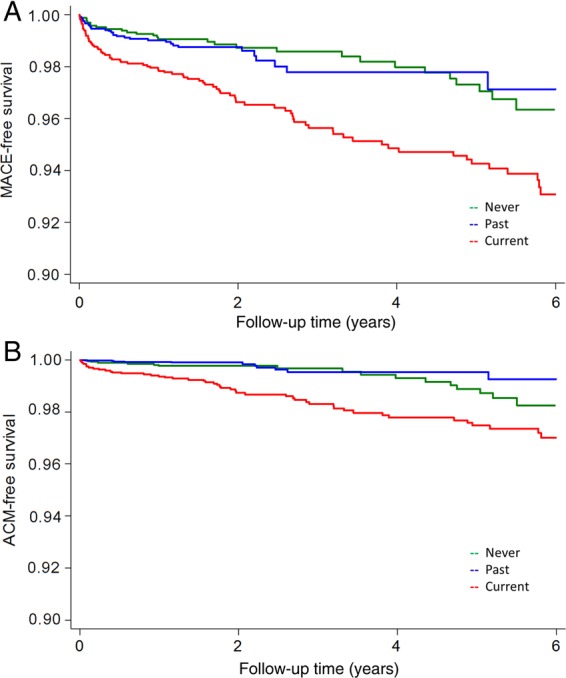
Methods and results: We evaluated 9456 patients (57.1 ± 12.3 years, 55.5% male) without known CAD (1588 current smokers; 2183 past smokers who quit ≥3 months before CCTA; and 5685 never smokers). By risk-adjusted Cox proportional-hazards models, we related smoking status to MACE (all-cause death or non-fatal myocardial infarction). We further performed 1:1:1 propensity matching for 1000 in each group evaluate event risk among individuals with similar age, gender, CAD risk factors, and symptom presentation. During a mean follow-up of 2.8 ± 1.9 years, 297 MACE occurred. Compared with never smokers, current and past smokers had greater atherosclerotic burden including extent of plaque defined as segments with any plaque (2.1 ± 2.8 vs. 2.6 ± 3.2 vs. 3.1 ± 3.3, P < 0.0001) and prevalence of obstructive CAD [1-vessel disease (VD): 10.6% vs. 14.9% vs. 15.2%, P < 0.001; 2-VD: 4.4% vs. 6.1% vs. 6.2%, P = 0.001; 3-VD: 3.1% vs. 5.2% vs. 4.3%, P < 0.001]. Compared with never smokers, current smokers experienced higher MACE risk [hazard ratio (HR) 1.9, 95% confidence interval (CI) 1.4-2.6, P < 0.001], while past smokers did not (HR 1.2, 95% CI 0.8-1.6, P = 0.35). Among matched individuals, current smokers had higher MACE risk (HR 2.6, 95% CI 1.6-4.2, P < 0.001), while past smokers did not (HR 1.3, 95% CI 0.7-2.4, P = 0.39). Similar findings were observed for risk of all-cause death.
Conclusion: Among patients without known CAD undergoing CCTA, current and past smokers had increased burden of atherosclerosis compared with never smokers; however, risk of MACE was heightened only in current smokers.
Keywords: Coronary atherosclerosis; Coronary computed tomographic angiography; Major adverse cardiovascular risk; Smoking risk.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
Risk factors. Smoking and CAD--what's plaque got to do with it?Nat Rev Cardiol. 2015 May;12(5):265-6. doi: 10.1038/nrcardio.2015.37. Epub 2015 Mar 31. Nat Rev Cardiol. 2015. PMID: 25824517 No abstract available.
References
-
- McEvoy JW, Blaha MJ, Rivera JJ, Budoff MJ, Khan AN, Shaw LJ, Berman DS, Raggi P, Min JK, Rumberger JA, Callister TQ, Blumenthal RS, Nasir K. Mortality rates in smokers and nonsmokers in the presence or absence of coronary artery calcification. JACC Cardiovasc Imaging 2012;5:1037–1045. - PMC - PubMed
-
- Shaw LJ, Raggi P, Callister TQ, Berman DS. Prognostic value of coronary artery calcium screening in asymptomatic smokers and non-smokers. Eur Heart J 2006;27:968–975. - PubMed
-
- Musallam KM, Rosendaal FR, Zaatari G, Soweid A, Hoballah JJ, Sfeir PM, Zeineldine S, Tamim HM, Richards T, Spahn DR, Lotta LA, Peyvandi F, Jamali FR. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg 2013;148:755–762. - PubMed
-
- Suskin N, Sheth T, Negassa A, Yusuf S. Relationship of current and past smoking to mortality and morbidity in patients with left ventricular dysfunction. J Am Coll Cardiol 2001;37:1677–1682. - PubMed
-
- Hasdai D, Garratt KN, Grill DE, Lerman A, Holmes DR. Effect of smoking status on the long-term outcome after successful percutaneous coronary revascularization. N Engl J Med 1997;336:755–761. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
