

Genomic classifier identifies men with adverse pathology after radical prostatectomy who benefit from adjuvant radiation therapy
- PMID: 25667284
- PMCID: PMC4884273
- DOI: 10.1200/JCO.2014.59.0026
Genomic classifier identifies men with adverse pathology after radical prostatectomy who benefit from adjuvant radiation therapy
Erratum in
-
Errata.J Clin Oncol. 2015 Apr 20;33(12):1416. doi: 10.1200/jco.2015.61.9759. J Clin Oncol. 2015. PMID: 25883365 Free PMC article. No abstract available.
Abstract
Purpose: The optimal timing of postoperative radiotherapy (RT) after radical prostatectomy (RP) is unclear. We hypothesized that a genomic classifier (GC) would provide prognostic and predictive insight into the development of clinical metastases in men receiving post-RP RT and inform decision making.
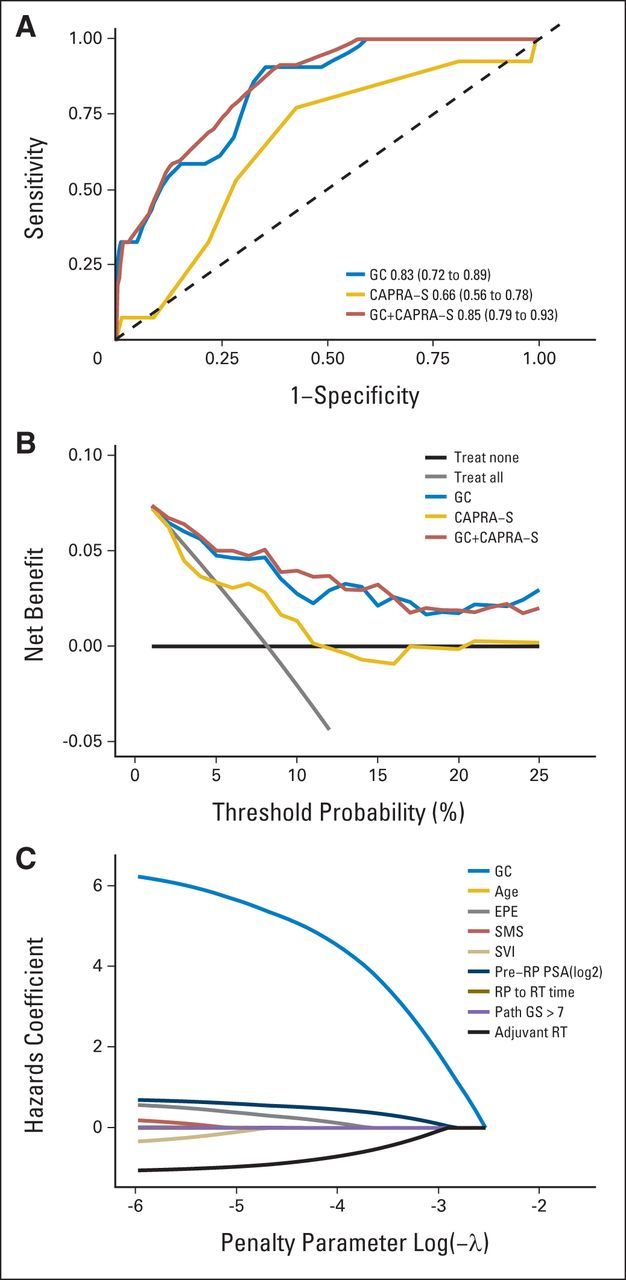
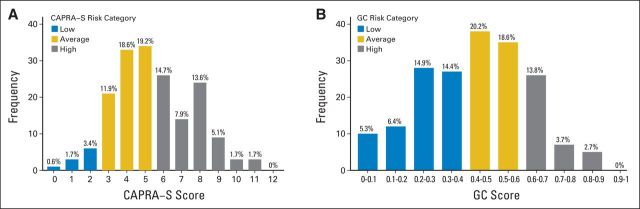
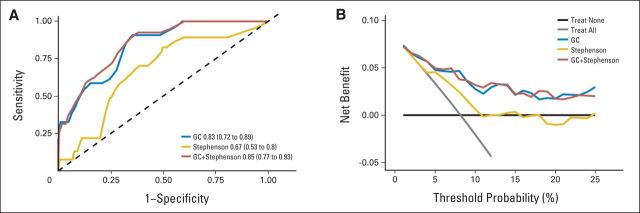
Patients and methods: GC scores were calculated from 188 patients with pT3 or margin-positive prostate cancer, who received post-RP RT at Thomas Jefferson University and Mayo Clinic between 1990 and 2009. The primary end point was clinical metastasis. Prognostic accuracy of the models was tested using the concordance index for censored data and decision curve analysis. Cox regression analysis tested the relationship between GC and metastasis.
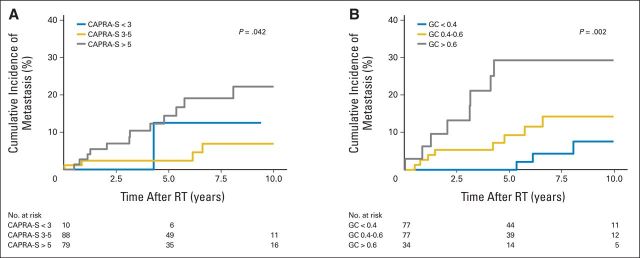
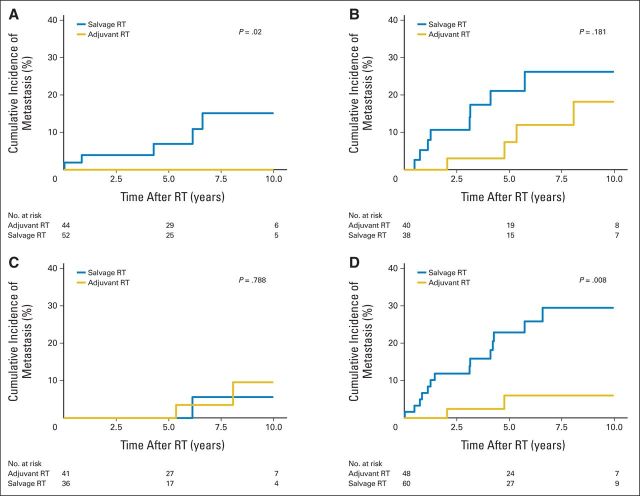
Results: The cumulative incidence of metastasis at 5 years after RT was 0%, 9%, and 29% for low, average, and high GC scores, respectively (P = .002). In multivariable analysis, GC and pre-RP prostate-specific antigen were independent predictors of metastasis (both P < .01). Within the low GC score (< 0.4), there were no differences in the cumulative incidence of metastasis comparing patients who received adjuvant or salvage RT (P = .79). However, for patients with higher GC scores (≥ 0.4), cumulative incidence of metastasis at 5 years was 6% for patients treated with adjuvant RT compared with 23% for patients treated with salvage RT (P < .01).
Conclusion: In patients treated with post-RP RT, GC is prognostic for the development of clinical metastasis beyond routine clinical and pathologic features. Although preliminary, patients with low GC scores are best treated with salvage RT, whereas those with high GC scores benefit from adjuvant therapy. These findings provide the first rational selection of timing for post-RP RT.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
The need for a personalized approach for prostate cancer management.BMC Med. 2015 May 9;13:109. doi: 10.1186/s12916-015-0344-1. BMC Med. 2015. PMID: 25956920 Free PMC article.
-
Re: Genomic Classifier Identifies Men with Adverse Pathology After Radical Prostatectomy Who Benefit from Adjuvant Radiation Therapy.Eur Urol. 2015 Aug;68(2):337-8. doi: 10.1016/j.eururo.2015.03.014. Eur Urol. 2015. PMID: 26149727 No abstract available.
-
Words of Wisdom. Re: Genomic Classifier Identifies Men with Adverse Pathology After Radical Prostatectomy Who Benefit from Adjuvant Radiation Therapy.Eur Urol. 2016 Mar;69(3):539-40. doi: 10.1016/j.eururo.2015.12.026. Eur Urol. 2016. PMID: 26867726 No abstract available.
References
-
- Cary KC, Paciorek A, Fuldeore MJ, et al. Temporal trends and predictors of salvage cancer treatment after failure following radical prostatectomy or radiation therapy: An analysis from the CaPSURE registry. Cancer. 2014;120:507–512. - PubMed
-
- Ost P, De Troyer B, Fonteyne V, et al. A matched control analysis of adjuvant and salvage high-dose postoperative intensity-modulated radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2011;80:1316–1322. - PubMed
-
- Briganti A, Wiegel T, Joniau S, et al. Early salvage radiation therapy does not compromise cancer control in patients with pT3N0 prostate cancer after radical prostatectomy: Results of a match-controlled multi-institutional analysis. Eur Urol. 2012;62:472–487. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
