

Does aggressive surgery improve outcomes? Interaction between preoperative disease burden and complex surgery in patients with advanced-stage ovarian cancer: an analysis of GOG 182
- PMID: 25667285
- PMCID: PMC4348639
- DOI: 10.1200/JCO.2014.56.3106
Does aggressive surgery improve outcomes? Interaction between preoperative disease burden and complex surgery in patients with advanced-stage ovarian cancer: an analysis of GOG 182
Abstract
Purpose: To examine the effects of disease burden, complex surgery, and residual disease (RD) status on progression-free (PFS) and overall survival (OS) in patients with advanced epithelial ovarian cancer (EOC) or primary peritoneal cancer (PPC) and complete surgical resection (R0) or < 1 cm of RD (MR) after surgical cytoreduction.
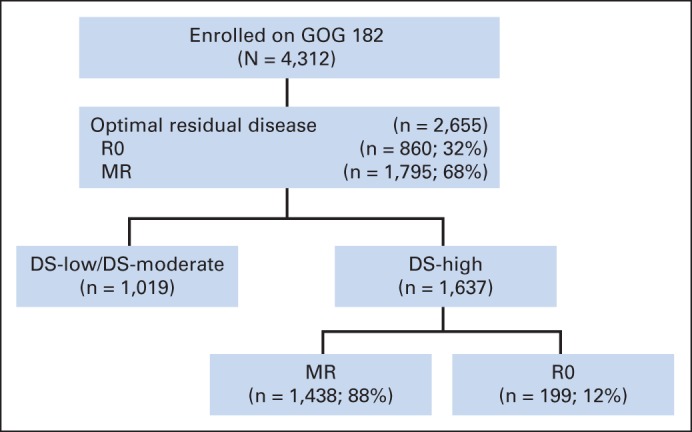
Patients and methods: Demographic, pathologic, surgical, and outcome data were collected from 2,655 patients with EOC or PPC enrolled onto the Gynecologic Oncology Group 182 study. The effects of disease distribution (disease score [DS]) and complexity of surgery (complexity score [CS]) on PFS and OS were assessed using the Kaplan-Meier method and multivariable regression analysis.
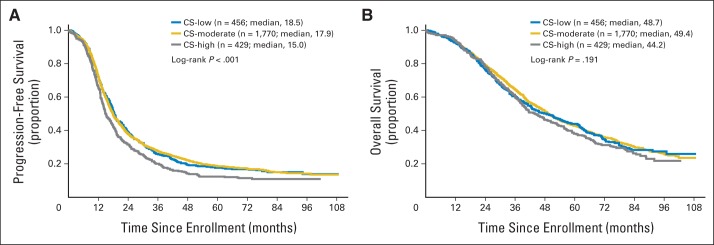
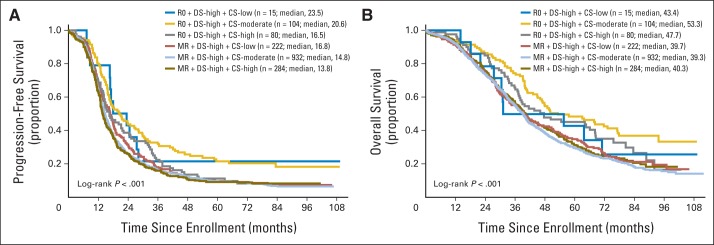
Results: Consistent with existing literature, patients with MR had worse prognosis than R0 patients (PFS, 15 v 29 months; P < .01; OS, 41 v 77 months; P < .01). Patients with the highest preoperative disease burden (DS high) had shorter PFS (15 v 23 or 34 months; P < .01) and OS (40 v 71 or 86 months; P < .01) compared with those with DS moderate or low, respectively. This relationship was maintained in the subset of R0 patients with PFS (18.3 v 33.2 months; DS moderate or low: P < .001) and OS (50.1 v 82.8 months; DS moderate or low: P < .001). After controlling for DS, RD, an interaction term for DS/CS, performance status, age, and cell type, CS was not an independent predictor of either PFS or OS.
Conclusion: In this large multi-institutional sample, initial disease burden remained a significant prognostic indicator despite R0. Complex surgery does not seem to affect survival when accounting for other confounding influences, particularly RD.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures



Comment in
-
Reply to G.D. Aletti et al.J Clin Oncol. 2015 Oct 20;33(30):3521-2. doi: 10.1200/JCO.2015.62.5707. Epub 2015 Aug 24. J Clin Oncol. 2015. PMID: 26304879 No abstract available.
-
There Is Nothing New Under the Sun.J Clin Oncol. 2015 Oct 20;33(30):3520. doi: 10.1200/JCO.2015.61.9536. Epub 2015 Aug 24. J Clin Oncol. 2015. PMID: 26304883 No abstract available.
-
The impact of splenectomy and diaphragmatic surgery on perioperative morbidity and overall survival of ovarian cancer patients.Ginekol Pol. 2023;94(10):807-815. doi: 10.5603/GP.a2023.0028. Epub 2023 Mar 17. Ginekol Pol. 2023. PMID: 36929791
References
-
- Siegel R, Naishadham D, Jemal A. Cancer Statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Reis LAG, Eisner MP, Kosary CL, et al., editors. SEER Cancer Statistics Review, 1975-2001. http://www.seer.cancer.gov/csr/1975_2001/
-
- Makar AP, Baekelandt M, Tropé CG, et al. The prognostic significance of residual disease, FIGO substage, tumor histology, and grade in patients with FIGO stage III ovarian cancer. Gynecol Oncol. 1995;56:175–180. - PubMed
-
- Eisenkop SM, Friedman RL, Wang H. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: A prospective study. Gynecol Oncol. 1998;69:103–106. - PubMed
-
- Eisenkop SM, Spirtos NM. Procedures required to accomplish complete cytoreduction of ovarian cancer: Is there a correlation with “biological aggressiveness” and survival? Gynecol Oncol. 2001;82:435–441. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
