

Phase II Trial of Graft-versus-Host Disease Prophylaxis with Post-Transplantation Cyclophosphamide after Reduced-Intensity Busulfan/Fludarabine Conditioning for Hematological Malignancies
- PMID: 25667989
- PMCID: PMC4825327
- DOI: 10.1016/j.bbmt.2015.01.026
Phase II Trial of Graft-versus-Host Disease Prophylaxis with Post-Transplantation Cyclophosphamide after Reduced-Intensity Busulfan/Fludarabine Conditioning for Hematological Malignancies
Abstract
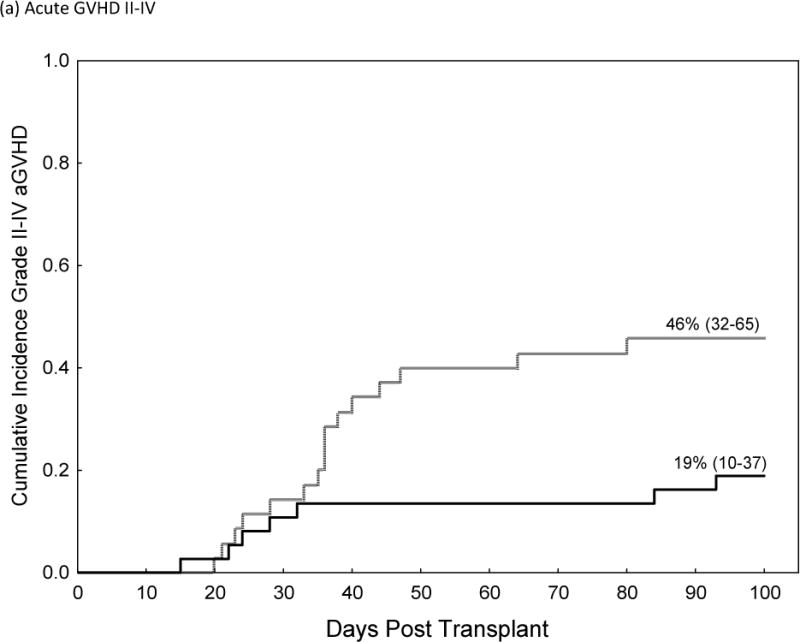
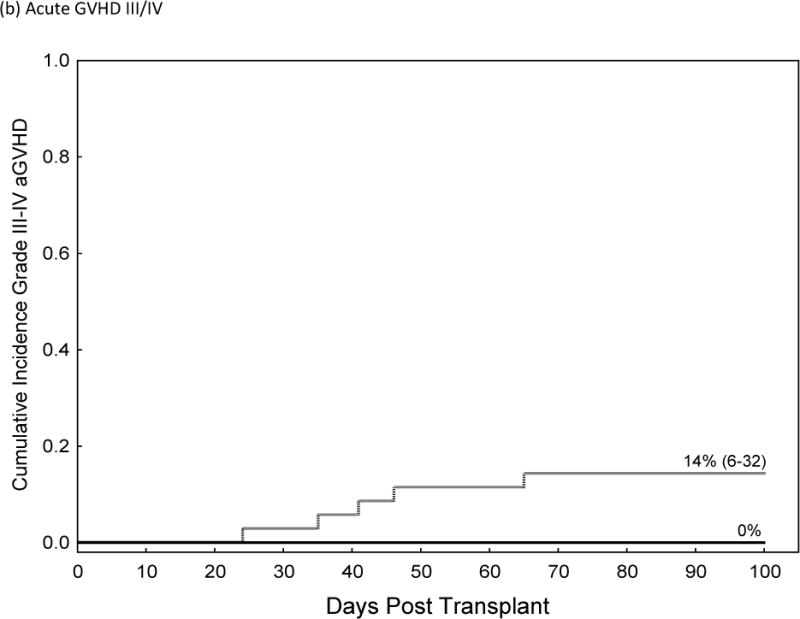
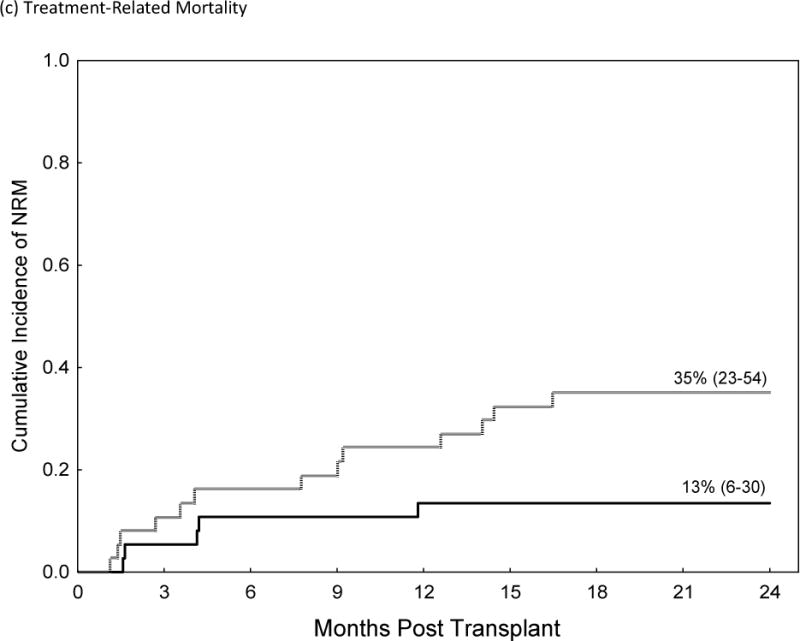
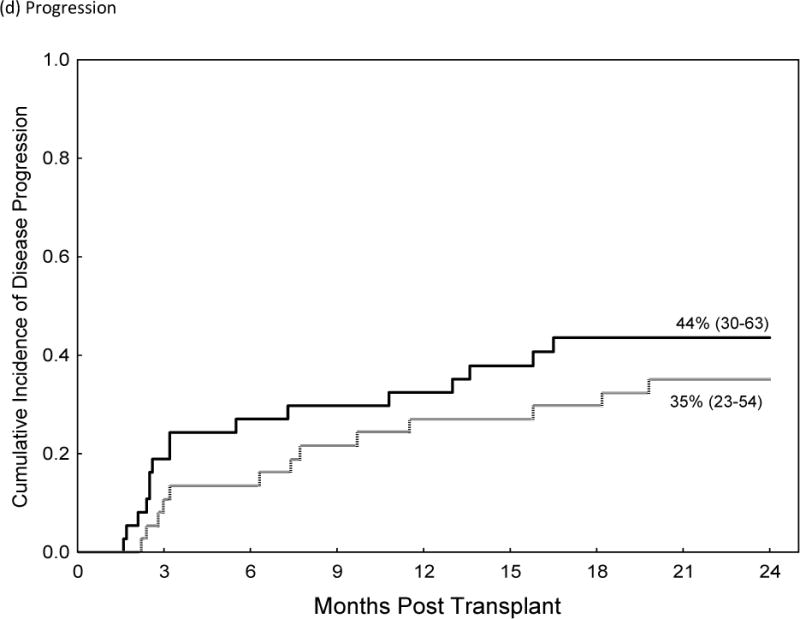
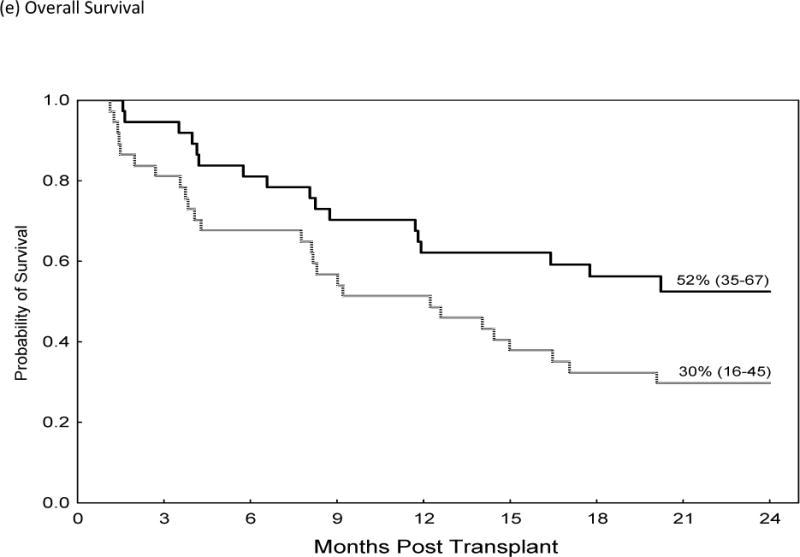
Graft-versus-host disease (GVHD) prophylaxis with post-transplantation cyclophosphamide (CY) after ablative HLA-matched bone marrow (BM) transplantation has been reported to have comparable rates of acute GVHD with an apparent reduction in chronic GVHD and infections when compared to historical prophylaxis with a calcineurin-inhibitor (CNI) and methotrexate (MTX). We conducted a phase II trial of post-transplantation CY (post-CY) after reduced-intensity conditioning (RIC) using intravenous busulfan (area under the curve of 4000 micromolar minute), fludarabine (40 mg/m(2)) for 4 days, and CY 50 mg/kg on days +3 and +4 after BM or peripheral blood (PB) transplantations from matched related (MRD) or unrelated donors (MUD). MUD recipients received antithymocyte globulin (ATG); however, a later amendment removed ATG. Forty-nine patients were treated (acute myeloid leukemia/myelodysplastic syndrome, 82%). Median age was 62 years (range, 39 to 72). Fifteen patients received an MRD (9 PB/6 BM); 34 had a MUD (2 PB/32 BM). The cumulative incidence of grade II to IV acute GVHD, III to IV acute GVHD, and chronic GVHD was 58%, 22%, and 18%, respectively. A matched cohort analysis compared outcomes to tacrolimus/methotrexate GVHD prophylaxis and indicated higher rates of acute GVHD grade II to IV (46% versus 19%; hazard ratio [HR], 2.8; P = .02) and treatment-related mortality (HR, 3.3; P = .035) and worse overall survival (HR, 1.9; P = .04) with post-CY. The incidence of chronic GVHD and CMV reactivation did not differ. This study suggests that post-CY should not be used as sole GVHD prophylaxis after a RIC transplantation from HLA-matched donors.
Keywords: Acute; Chronic; Graft-versus-host disease; Marrow; Stem cell transplantation.
Copyright © 2015 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Li Y, Li XC, Zheng XX, Wells AD, Turka LA, Strom TB. Blocking both signal 1 and signal 2 of T-cell activation prevents apoptosis of alloreactive T cells and induction of peripheral allograft tolerance. Nature medicine. 1999;5(11):1298–1302. doi: 10.1038/15256. e-pub ahead of print 1999/11/05. - DOI - PubMed
-
- Fischer AC, Ruvolo PP, Burt R, Horwitz LR, Bright EC, Hess JM, et al. Characterization of the autoreactive T cell repertoire in cyclosporin-induced syngeneic graft-versus-host disease. A highly conserved repertoire mediates autoaggression. Journal of immunology (Baltimore, Md: 1950) 1995;154(8):3713–3725. e-pub ahead of print 1995/04/15. - PubMed
-
- Beschorner WE, Hess AD, Shinn CA, Santos GW. Transfer of cyclosporine-associated syngeneic graft-versus-host disease by thymocytes. Resemblance to chronic graft-versus-host disease. Transplantation. 1988;45(1):209–215. e-pub ahead of print 1988/01/01. - PubMed
-
- Jenkins MK, Schwartz RH, Pardoll DM. Effects of cyclosporine A on T cell development and clonal deletion. Science. 1988;241(4873):1655–1658. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
