

Oral iron supplementation after blood donation: a randomized clinical trial
- PMID: 25668261
- PMCID: PMC5094173
- DOI: 10.1001/jama.2015.119
Oral iron supplementation after blood donation: a randomized clinical trial
Abstract
Importance: Although blood donation is allowed every 8 weeks in the United States, recovery of hemoglobin to the currently accepted standard (12.5 g/dL) is frequently delayed, and some donors become anemic.
Objective: To determine the effect of oral iron supplementation on hemoglobin recovery time (days to recovery of 80% of hemoglobin removed) and recovery of iron stores in iron-depleted ("low ferritin," ≤26 ng/mL) and iron-replete ("higher ferritin," >26 ng/mL) blood donors.
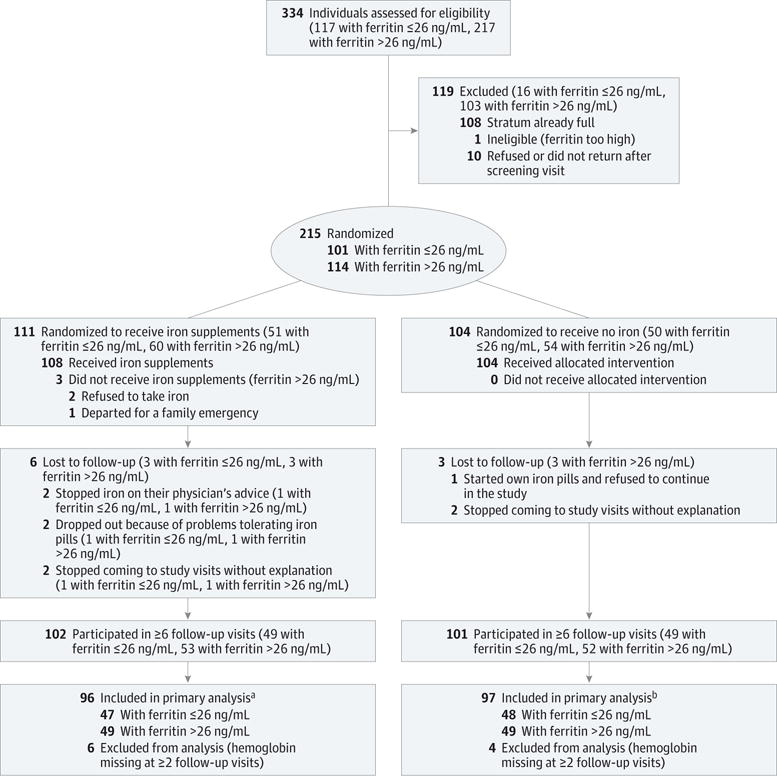
Design, setting, and participants: Randomized, nonblinded clinical trial of blood donors stratified by ferritin level, sex, and age conducted in 4 regional blood centers in the United States in 2012. Included were 215 eligible participants aged 18 to 79 years who had not donated whole blood or red blood cells within 4 months.
Interventions: One tablet of ferrous gluconate (37.5 mg of elemental iron) daily or no iron for 24 weeks (168 days) after donating a unit of whole blood (500 mL).
Main outcomes and measures: Time to recovery of 80% of the postdonation decrease in hemoglobin and recovery of ferritin level to baseline as a measure of iron stores.
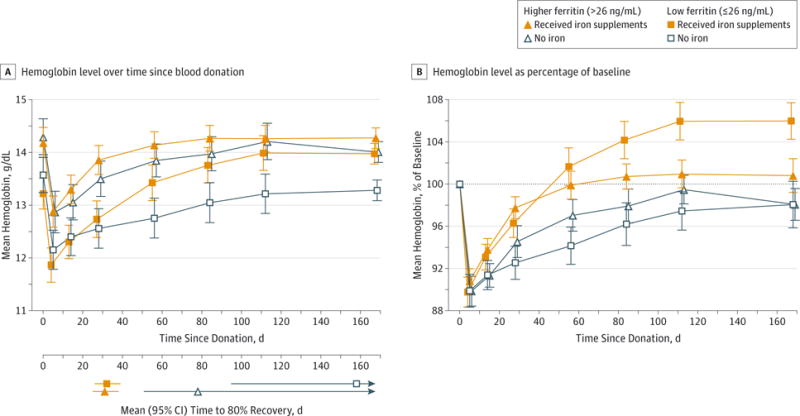
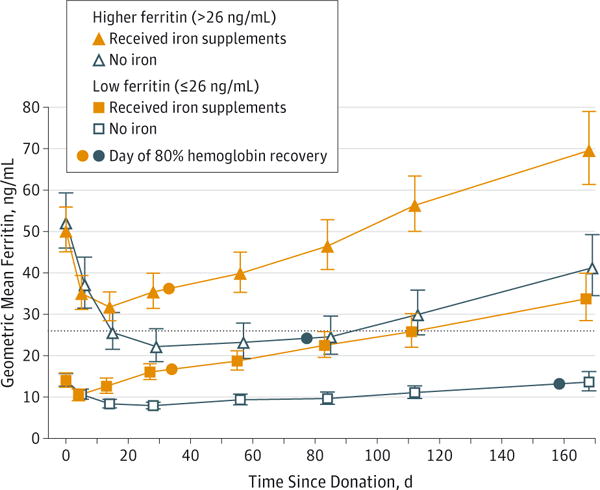
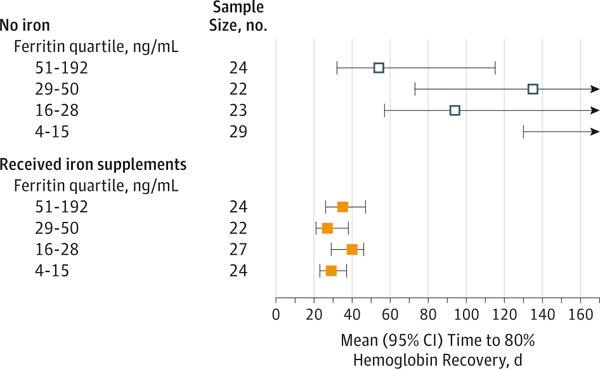
Results: The mean baseline hemoglobin levels were comparable in the iron and no-iron groups and declined from a mean (SD) of 13.4 (1.1) g/dL to 12.0 (1.2) g/dL after donation in the low-ferritin group and from 14.2 (1.1) g/dL to 12.9 (1.2) g/dL in the higher-ferritin group. Compared with participants who did not receive iron supplementation, those who received iron supplementation had shortened time to 80% hemoglobin recovery in both the low-ferritin (mean, 32 days, interquartile range [IQR], 30-34, vs 158 days, IQR, 126->168) and higher-ferritin groups (31 days, IQR, 29-33, vs 78 days, IQR, 66-95). Median time to recovery to baseline ferritin levels in the low-ferritin group taking iron was 21 days (IQR, 12-84). For participants not taking iron, recovery to baseline was longer than 168 days (IQR, 128->168). Median time to recovery to baseline in the higher-ferritin group taking iron was 107 days (IQR, 75-141), and for participants not taking iron, recovery to baseline was longer than 168 days (IQR, >168->168). Recovery of iron stores in all participants who received supplements took a median of 76 days (IQR, 20-126); for participants not taking iron, median recovery time was longer than 168 days (IQR, 147->168 days; P < .001). Without iron supplements, 67% of participants did not recover iron stores by 168 days.
Conclusions and relevance: Among blood donors with normal hemoglobin levels, low-dose iron supplementation, compared with no supplementation, reduced time to 80% recovery of the postdonation decrease in hemoglobin concentration in donors with low ferritin (≤26 ng/mL) or higher ferritin (>26 ng/mL).
Trial registration: clinicaltrials.gov Identifier: NCT01555060.
Conflict of interest statement
Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mast reported having received a grant from Novo Nordisk and honoraria from Siemens. No other disclosures were reported.
Figures
References
-
- Baart AM, van Noord PAH, Vergouwe Y, et al. High prevalence of subclinical iron deficiency in whole blood donors not deferred for low hemoglobin. Transfusion. 2013;53(8):1670–1677. - PubMed
-
- Whitaker BI, Hinkins S. 2011 National blood collection and utilization survey report. US Dept of Health and Human Services; http://www.hhs.gov/ash/bloodsafety/2011-nbcus.pdf. Accessed November 25, 2014.
-
- Krayenbuehl PA, Battegay E, Breymann C, Furrer J, Schulthess G. Intravenous iron for the treatment of fatigue in nonanemic, premenopausal women with low serum ferritin concentration. Blood. 2011;118(12):3222–3227. - PubMed
-
- Brownlie T, IV, Utermohlen V, Hinton PS, Haas JD. Tissue iron deficiency without anemia impairs adaptation in endurance capacity after aerobic training in previously untrained women. Am J Clin Nutr. 2004;79(3):437–443. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HHSN268201100001I/HL/NHLBI NIH HHS/United States
- HHSN268201100003C/WH/WHI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100001I/HL/NHLBI NIH HHS/United States
- HHSN268201100002C/WH/WHI NIH HHS/United States
- HHSN268201100004I/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100003I/HL/NHLBI NIH HHS/United States
- HHSN268201100002I/HL/NHLBI NIH HHS/United States
- HHSN268201100001C/WH/WHI NIH HHS/United States
- HHSN268201100003I/HL/NHLBI NIH HHS/United States
- HHSN268201100002I/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100004I/HL/NHLBI NIH HHS/United States
- HHSN268201100004C/WH/WHI NIH HHS/United States
- HHSN268201100006I/PHS HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
