

Effect of creatine monohydrate on clinical progression in patients with Parkinson disease: a randomized clinical trial
- PMID: 25668262
- PMCID: PMC4349346
- DOI: 10.1001/jama.2015.120
Effect of creatine monohydrate on clinical progression in patients with Parkinson disease: a randomized clinical trial
Abstract
Importance: There are no treatments available to slow or prevent the progression of Parkinson disease, despite its global prevalence and significant health care burden. The National Institute of Neurological Disorders and Stroke Exploratory Trials in Parkinson Disease program was established to promote discovery of potential therapies.
Objective: To determine whether creatine monohydrate was more effective than placebo in slowing long-term clinical decline in participants with Parkinson disease.
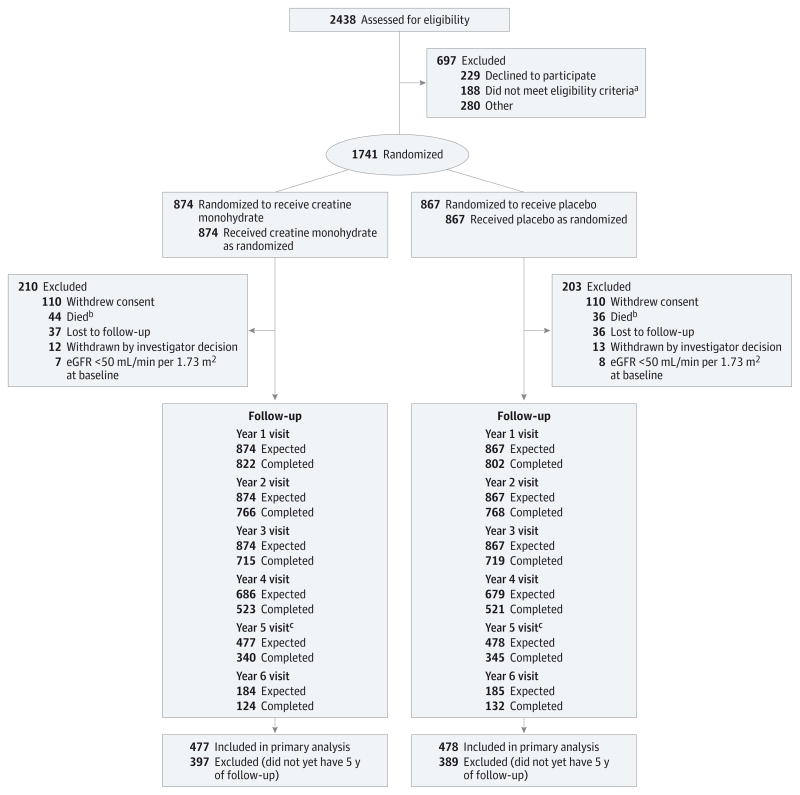
Design, setting, and patients: The Long-term Study 1, a multicenter, double-blind, parallel-group, placebo-controlled, 1:1 randomized efficacy trial. Participants were recruited from 45 investigative sites in the United States and Canada and included 1741 men and women with early (within 5 years of diagnosis) and treated (receiving dopaminergic therapy) Parkinson disease. Participants were enrolled from March 2007 to May 2010 and followed up until September 2013.
Interventions: Participants were randomized to placebo or creatine (10 g/d) monohydrate for a minimum of 5 years (maximum follow-up, 8 years).
Main outcomes and measures: The primary outcome measure was a difference in clinical decline from baseline to 5-year follow-up, compared between the 2 treatment groups using a global statistical test. Clinical status was defined by 5 outcome measures: Modified Rankin Scale, Symbol Digit Modalities Test, PDQ-39 Summary Index, Schwab and England Activities of Daily Living scale, and ambulatory capacity. All outcomes were coded such that higher scores indicated worse outcomes and were analyzed by a global statistical test. Higher summed ranks (range, 5-4775) indicate worse outcomes.
Results: The trial was terminated early for futility based on results of a planned interim analysis of participants enrolled at least 5 years prior to the date of the analysis (n = 955). The median follow-up time was 4 years. Of the 955 participants, the mean of the summed ranks for placebo was 2360 (95% CI, 2249-2470) and for creatine was 2414 (95% CI, 2304-2524). The global statistical test yielded t1865.8 = -0.75 (2-sided P = .45). There were no detectable differences (P < .01 to partially adjust for multiple comparisons) in adverse and serious adverse events by body system.
Conclusions and relevance: Among patients with early and treated Parkinson disease, treatment with creatine monohydrate for at least 5 years, compared with placebo did not improve clinical outcomes. These findings do not support the use of creatine monohydrate in patients with Parkinson disease.
Trial registration: clinicaltrials.gov Identifier: NCT00449865.
Conflict of interest statement
Figures
References
-
- Dorsey ER, Constantinescu R, Thompson JP, et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology. 2007;68(5):384–386. - PubMed
-
- Kowal SL, Dall TM, Chakrabarti R, Storm MV, Jain A. The current and projected economic burden of Parkinson’s disease in the United States. Mov Disord. 2013;28(3):311–318. - PubMed
-
- Ravina BM, Fagan SC, Hart RG, et al. Neuroprotective agents for clinical trials in Parkinson’s disease: a systematic assessment. Neurology. 2003;60(8):1234–1240. - PubMed
-
- NINDS NET-PD Investigators. A randomized, double-blind, futility clinical trial of creatine and minocycline in early Parkinson disease. Neurology. 2006;66(5):664–671. - PubMed
-
- NINDS NET-PD Investigators. A randomized clinical trial of coenzyme Q10 and GPI-1485 in early Parkinson disease. Neurology. 2007;68(1):20–28. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- K12 NS066098/NS/NINDS NIH HHS/United States
- K23 AG034236/AG/NIA NIH HHS/United States
- U10 NS044460/NS/NINDS NIH HHS/United States
- NS44504-08/NS/NINDS NIH HHS/United States
- U10 NS044545/NS/NINDS NIH HHS/United States
- U01NS43128/NS/NINDS NIH HHS/United States
- P50 NS091856/NS/NINDS NIH HHS/United States
- U10 NS044504/NS/NINDS NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- U01 NS043128/NS/NINDS NIH HHS/United States
- R24 MD001779/MD/NIMHD NIH HHS/United States
- K23 NS072283/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
