

Improving selection criteria for lung cancer screening. The potential role of emphysema
- PMID: 25668622
- PMCID: PMC5447319
- DOI: 10.1164/rccm.201410-1848OC
Improving selection criteria for lung cancer screening. The potential role of emphysema
Abstract
Rationale: Lung cancer (LC) screening using low-dose chest computed tomography is now recommended in several guidelines using the National Lung Screening Trial (NLST) entry criteria (age, 55-74; ≥30 pack-years; tobacco cessation within the previous 15 yr for former smokers). Concerns exist about their lack of sensitivity.
Objectives: To evaluate the performance of NLST criteria in two different LC screening studies from Europe and the United States, and to explore the effect of using emphysema as a complementary criterion.
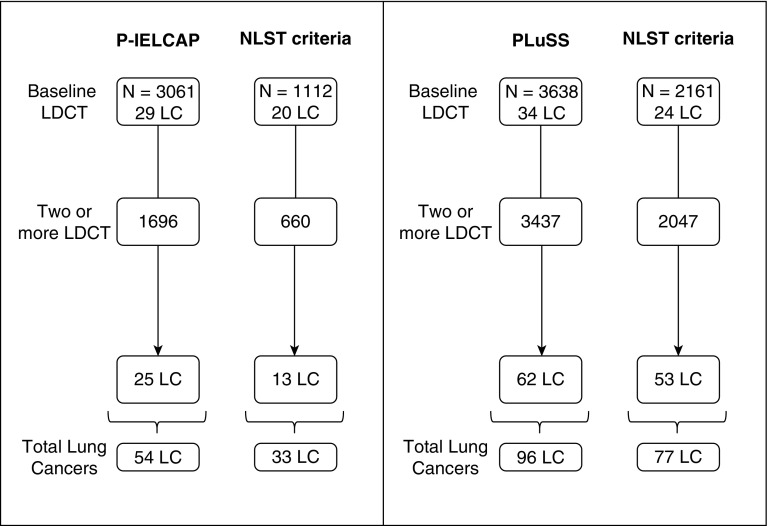
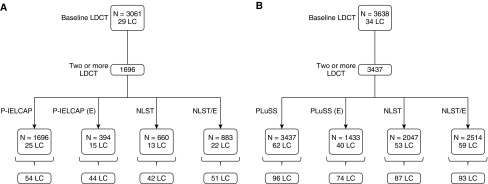
Methods: Participants from the Pamplona International Early Lung Action Detection Program (P-IELCAP; n = 3,061) and the Pittsburgh Lung Screening Study (PLuSS; n = 3,638) were considered. LC cumulative frequencies, incidence densities, and annual detection rates were calculated in three hypothetical cohorts, including subjects who met NLST criteria alone, those with computed tomography-detected emphysema, and those who met NLST criteria and/or had emphysema.
Measurements and main results: Thirty-six percent and 59% of P-IELCAP and PLuSS participants, respectively, met NLST criteria. Among these, higher LC incidence densities and detection rates were observed. However, applying NLST criteria to our original cohorts would miss as many as 39% of all LC. Annual screening of subjects meeting either NLST criteria or having emphysema detected most cancers (88% and 95% of incident LC of P-IELCAP and PLuSS, respectively) despite reducing the number of screened participants by as much as 52%.
Conclusions: LC screening based solely on NLST criteria could miss a significant number of LC cases. Combining NLST criteria and emphysema to select screening candidates results in higher LC detection rates and a lower number of cancers missed.
Keywords: National Lung Screening Trial; emphysema; low-dose computed tomography; lung cancer screening.
Figures

Comment in
-
Searching for red shirts. Emphysema as a lung cancer screening criterion?Am J Respir Crit Care Med. 2015 Apr 15;191(8):868-9. doi: 10.1164/rccm.201502-0381ED. Am J Respir Crit Care Med. 2015. PMID: 25876199 No abstract available.
References
-
- Humphrey LL, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP, Zakher B, Fu R, Slatore CG. Screening for lung cancer with low-dose computed tomography: a systematic review to update the US Preventive services task force recommendation. Ann Intern Med. 2013;159:411–420. - PubMed
-
- Field JK, Oudkerk M, Pedersen JH, Duffy SW. Prospects for population screening and diagnosis of lung cancer. Lancet. 2013;382:732–741. - PubMed
-
- American Lung AssociationProviding guidance on lung cancer screening to patients and physicians. 2012. Apr 23 [accessed 2013 Oct 17]. Available from: http://www.lung.org/lung-disease/lung-cancer/lung-cancer-screening- guid...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
