

Survival benefit of the primary prevention implantable cardioverter-defibrillator among older patients: does age matter? An analysis of pooled data from 5 clinical trials
- PMID: 25669833
- PMCID: PMC4408540
- DOI: 10.1161/CIRCOUTCOMES.114.001306
Survival benefit of the primary prevention implantable cardioverter-defibrillator among older patients: does age matter? An analysis of pooled data from 5 clinical trials
Abstract
Background: The impact of patient age on the risks of death or rehospitalization after primary prevention implantable cardioverter-defibrillator (ICD) placement is uncertain.
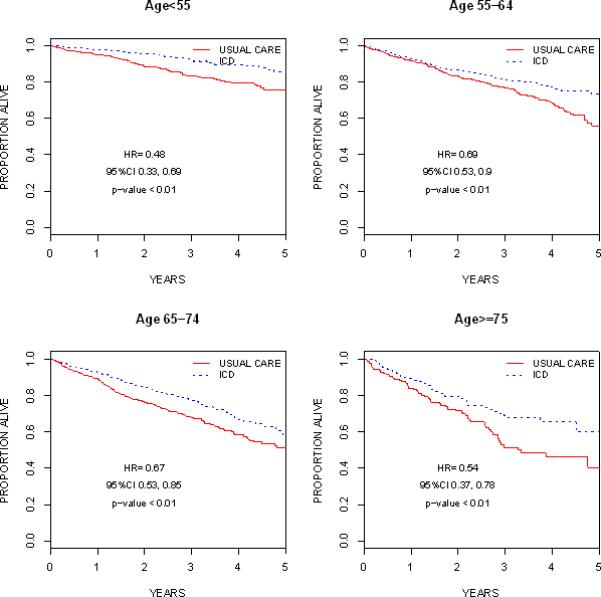
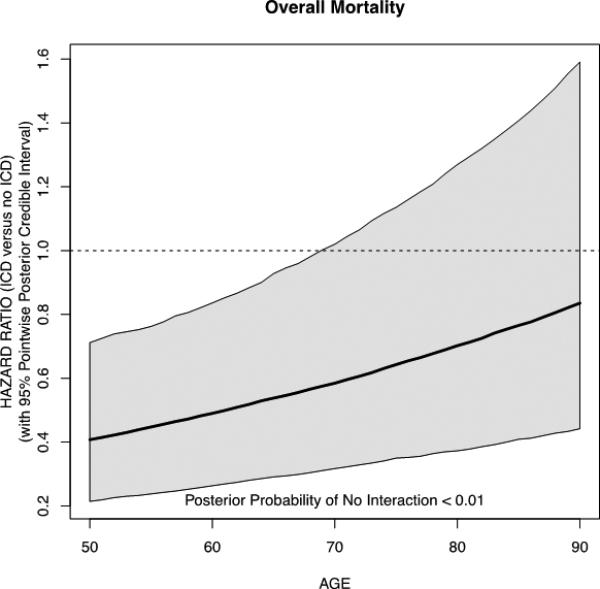
Methods and results: Data from 5 major ICD trials were merged: the Multicenter Automatic Defibrillator Implantation Trial I (MADIT-I), the Multicenter UnSustained Tachycardia Trial (MUSTT), the Multicenter Automatic Defibrillator Implantation Trial II (MADIT-II), the Defibrillators in Nonischemic Cardiomyopathy Treatment Evaluation Trial (DEFINITE), and the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Median age at enrollment was 62 (interquartile range 53-70) years. Compared with their younger counterparts, older patients had a greater burden of comorbid illness. In unadjusted exploratory analyses, ICD recipients were less likely to die than nonrecipients in all age groups: among patients aged <55 years: hazard ratio 0.48, 95% posterior credible interval 0.33 to 0.69; among patients aged 55 to 64 years: hazard ratio 0.69, 95% posterior credible interval 0.53 to 0.90; among patients aged 65 to 74 years: hazard ratio 0.67, 95% posterior credible interval, 0.53 to 0.85; and among patients aged ≥75 years: hazard ratio 0.54, 95% posterior credible interval 0.37 to 0.78. Sample sizes were limited among patients aged ≥75 years. In adjusted Bayesian-Weibull modeling, point estimates indicate ICD efficacy persists but is attenuated with increasing age. There was evidence of an interaction between age and ICD treatment on survival (two-sided posterior tail probability of no interaction <0.01). Using an adjusted Bayesian logistic regression model, there was no evidence of an interaction between age and ICD treatment on rehospitalization (two-sided posterior tail probability of no interaction 0.44).
Conclusions: In this analysis, the survival benefit of the ICD exists but is attenuated with increasing age. The latter finding may be because of the higher burden of comorbid illness, competing causes of death, or limited sample size of older patients. There was no evidence that age modifies the association between ICD treatment and rehospitalization.
Keywords: aging; defibrillators, implantable; meta-analysis.
© 2015 American Heart Association, Inc.
Figures
References
-
- Moss AJ, Hall J, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted cardioverterdefibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–40. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999;341:1882–90. - PubMed
-
- Moss AJ, Zareba W, Hall J, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- Kadish A, Dyer A, Daubert JP, Quigg R, Estes M, Anderson KP, Calkins H, Hoch D, Goldberg J, Shalaby A, Sanders WE, Schaechter A, Levine JH. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350:2151–8. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
