

Immunological response and overall survival in a subset of advanced renal cell carcinoma patients from a randomized phase 2/3 study of naptumomab estafenatox plus IFN-α versus IFN-α
- PMID: 25669986
- PMCID: PMC4414201
- DOI: 10.18632/oncotarget.2922
Immunological response and overall survival in a subset of advanced renal cell carcinoma patients from a randomized phase 2/3 study of naptumomab estafenatox plus IFN-α versus IFN-α
Abstract
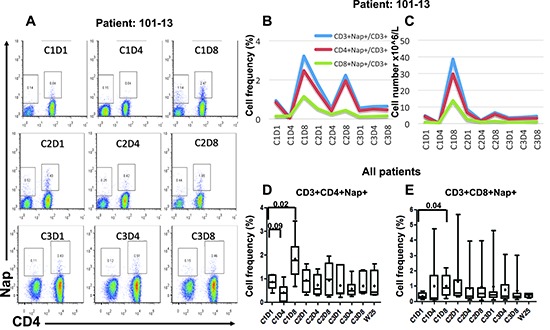
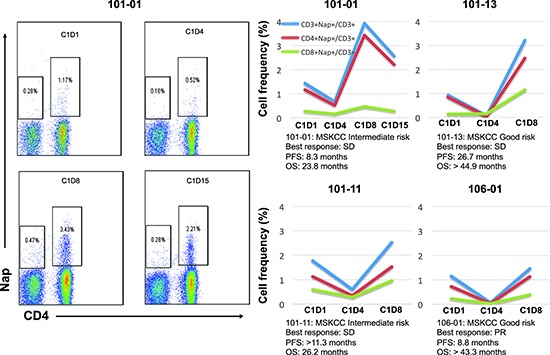
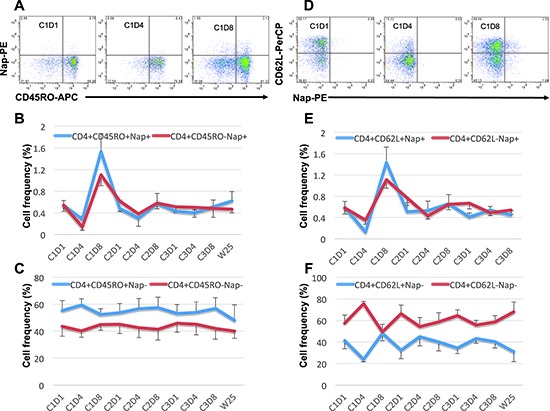
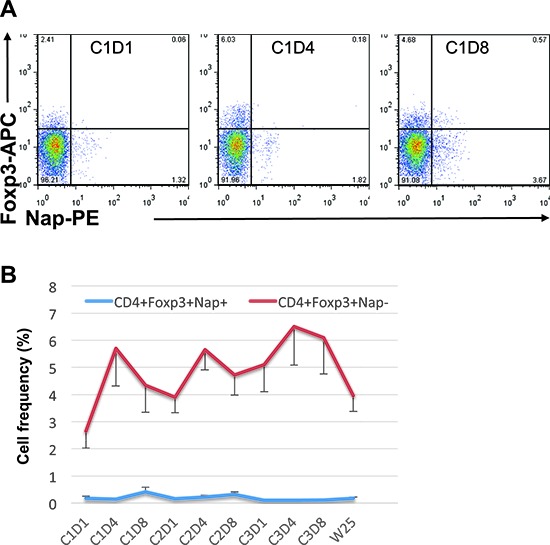
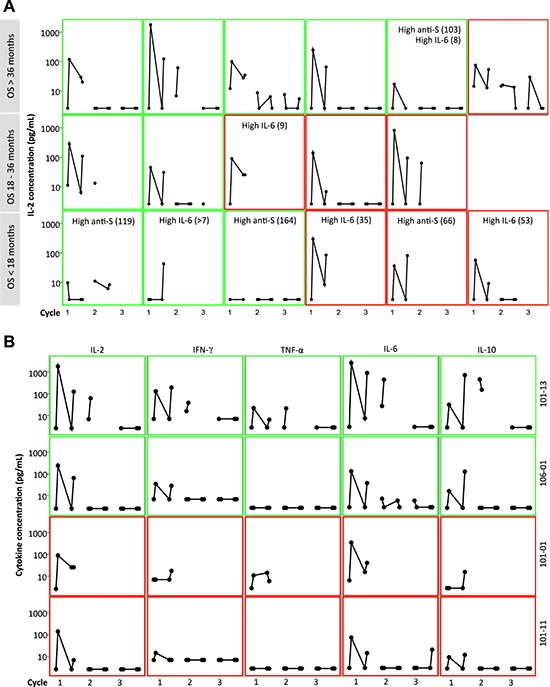
Naptumomab estafenatox/ABR-217620/ANYARA (Nap) has been evaluated in clinical phase 1 and 2/3 studies. RCC patients in the phase 2/3 trial were randomized 1:1 in an open label study to receive Nap+IFN-α or IFN-α. In this study, we analyzed the UK patients for their immunological response in relation to prolonged overall survival (OS). We found that Nap-specific T cells were reduced after 3 treatment days in patients' peripheral blood. Levels of both Nap-specific CD4+ and CD8+ T cells were significantly higher 8 days after the first treatment. Patients with such pattern of reduction and expansion of Nap-binding T cells also showed increased levels of IL-2 and IFN-γ in plasma 3 hours after the first Nap treatment. In addition, Nap caused an increase of IL-6, IL-10 and TNF-α. The patients in the UK subset showed a tendency of OS benefit after Nap treatment. Most Nap treated patients with long OS had low baseline IL-6 and normal levels of anti-SEA/E-120 antibodies. Furthermore, patients with pronounced Nap induced IL-2 and T cell expansion had long OS. In conclusion, patients with low baseline IL-6 and normal anti-SEA/E-120 may respond well to Nap by T cell activation and expansion paving the way for anti-tumour effects.
Conflict of interest statement
Anette Sundstedt, Örjan Nordle and Gunnar Hedlund are employees and hold shares in Active Biotech AB. Other authors have no conflict of interest.
Figures

References
-
- Abe H, Kamai T. Recent advances in the treatment of metastatic renal cell carcinoma. Int J Urol. 2013;20:944–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
