

doi: 10.1016/j.jash.2015.01.005.
Epub 2015 Jan 13.
Basic science: hypertensive target organ damage
- PMID: 25670252
- PMCID: PMC4369441
- DOI: 10.1016/j.jash.2015.01.005
Item in Clipboard
Basic science: hypertensive target organ damage
J Am Soc Hypertens.
2015 Mar.
No abstract available
Figures
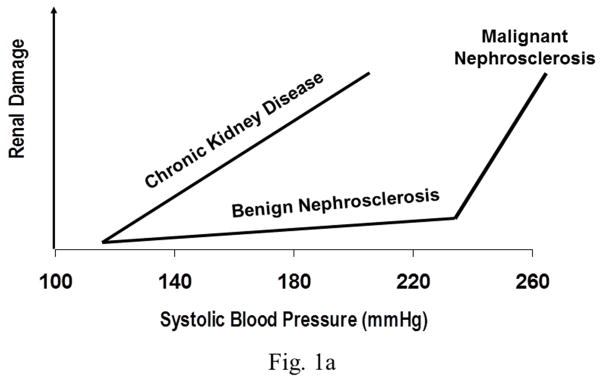
Fig. 1a. The differing BP thresholds and slopes of the relationship between BP
and renal damage in patients with uncomplicated hypertension (benign and
malignant nephrosclerosis) and those with diabetic and non-diabetic CKD. Fig. 1b. Illustration of the spectrum of pressure/flow relationships in the renal
vascular bed in hypertension. Pattern A represents the normal renal
autoregulatory responses observed in uncomplicated hypertension and shows the
constancy of renal blood flow (RBF) despite BP changes within the autoregulatory
range. Pattern B indicates the ambient renal vasodilation but preserved
autoregulation after uninephrectomy. Pattern C illustrates the impaired RBF
autoregulatory responses observed in the 5/6 renal ablation model. Pattern D
shows the complete loss of renal autoregulation in 5/6 renal ablated rats
treated with dihydropyridine CCBs. Although RBF is depicted as the dependent
variable, the same relationships are expected to obtain for glomerular
pressures, given that the autoregulatory resistance changes are confined to the
preglomerular vasculature.
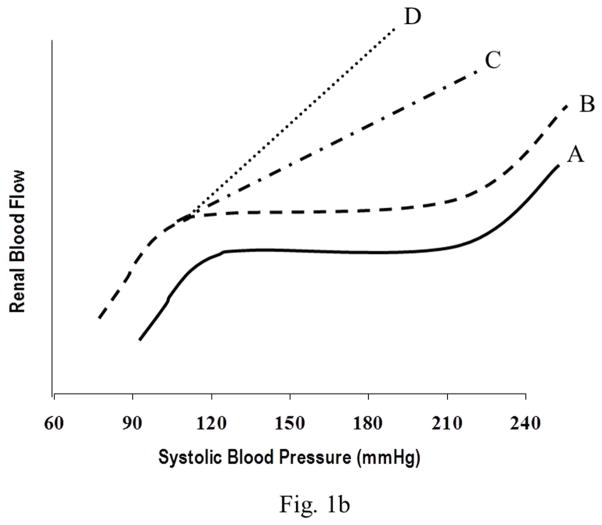
Fig. 1a. The differing BP thresholds and slopes of the relationship between BP
and renal damage in patients with uncomplicated hypertension (benign and
malignant nephrosclerosis) and those with diabetic and non-diabetic CKD. Fig. 1b. Illustration of the spectrum of pressure/flow relationships in the renal
vascular bed in hypertension. Pattern A represents the normal renal
autoregulatory responses observed in uncomplicated hypertension and shows the
constancy of renal blood flow (RBF) despite BP changes within the autoregulatory
range. Pattern B indicates the ambient renal vasodilation but preserved
autoregulation after uninephrectomy. Pattern C illustrates the impaired RBF
autoregulatory responses observed in the 5/6 renal ablation model. Pattern D
shows the complete loss of renal autoregulation in 5/6 renal ablated rats
treated with dihydropyridine CCBs. Although RBF is depicted as the dependent
variable, the same relationships are expected to obtain for glomerular
pressures, given that the autoregulatory resistance changes are confined to the
preglomerular vasculature.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
