

Abdominal cocoon syndrome is a rare cause of mechanical intestinal obstructions: a report of two cases
- PMID: 25671606
- PMCID: PMC4335564
- DOI: 10.12659/AJCR.892658
Abdominal cocoon syndrome is a rare cause of mechanical intestinal obstructions: a report of two cases
Abstract
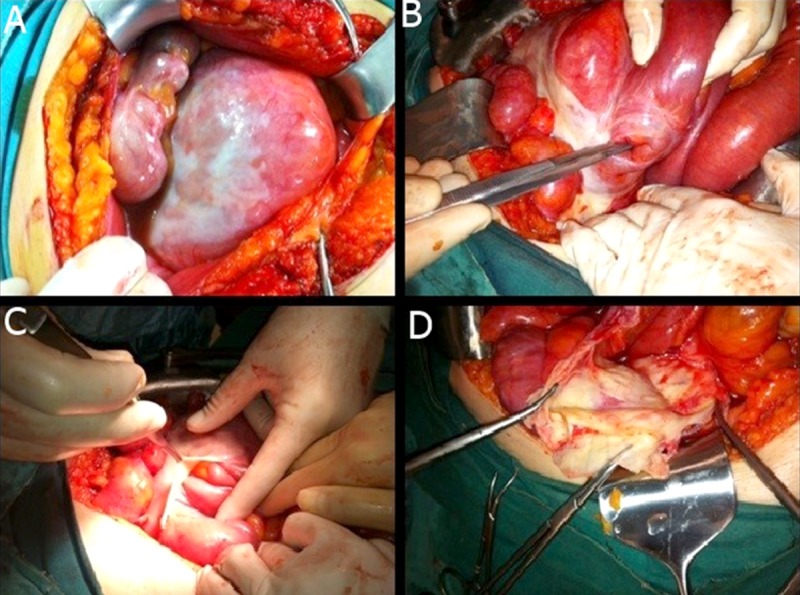
Background: Abdominal cocoon syndrome is also known in the literature as sclerosing peritonitis or sclerosing encapsulating peritonitis. It is characterized by total or partial encapsulation of abdominal viscera by a fibrous membrane. It has been reported mainly in adolescent women and the majority of the cases are of unknown etiology. Preoperative diagnosis is difficult and is usually established during laparotomy. We present 2 cases of acute mechanical intestinal obstruction caused by sclerosing encapsulating peritonitis.
Case report: Two male patients, ages 30 and 47, were admitted to our emergency department for mechanical intestinal obstruction. They were treated surgically and were diagnosed with abdominal cocoon syndrome.
Conclusions: If abdominal cocoon syndrome is diagnosed pre-operatively and acute abdomen symptoms are not observed, surgery is unnecessary. If surgery is inevitable, membrane resection and bridotomy must be performed, as in our 2 cases. If resection is going to be performed, primary anastomosis is not recommended. Iatrogenic injuries that happened during the operation should not be immediately repaired, because creation of the stoma from the proximal part of the injury is recommended.
Figures

References
-
- Foo KT, Ng KC, Rauff A, et al. Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. Br J Surg. 1978;65:427–30. - PubMed
-
- Salamone G, Atzeni J, Agrusa A, Gulotta G. A rare case of abdominal cocoon. Ann Ital Chir. 2013;pii:S2239253X13021531. 84(ePub) - PubMed
-
- Kumar A, Ramakrishanan TS, Sahu S, Mishra KB. Idiopatic sclerosing encapsulating peritonitis-is a preoperative diagnosis possiple? Report of 3 cases. Surg Today. 2009;39:610–14. - PubMed
-
- Pipitone N, Vaglio A, Salvarani C. Retroperitoneal fibrosis. Best Pract Res Clin Rheumatol. 2012;26:439–448. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
