

Prevalence and degree of thyroid pathology in hyperthyroid cats increases with disease duration: a cross-sectional analysis of 2096 cats referred for radioiodine therapy
- PMID: 25673019
- PMCID: PMC11149013
- DOI: 10.1177/1098612X15572416
Prevalence and degree of thyroid pathology in hyperthyroid cats increases with disease duration: a cross-sectional analysis of 2096 cats referred for radioiodine therapy
Abstract
Objectives: Hyperthyroidism is common in cats, but there are no reports that evaluate its severity or underlying thyroid tumor disease based on disease duration (ie, time from original diagnosis). The objective of this study was to compare serum thyroxine (T4) concentrations and thyroid scintigraphic characteristics of cats referred for radioiodine treatment based on disease duration.
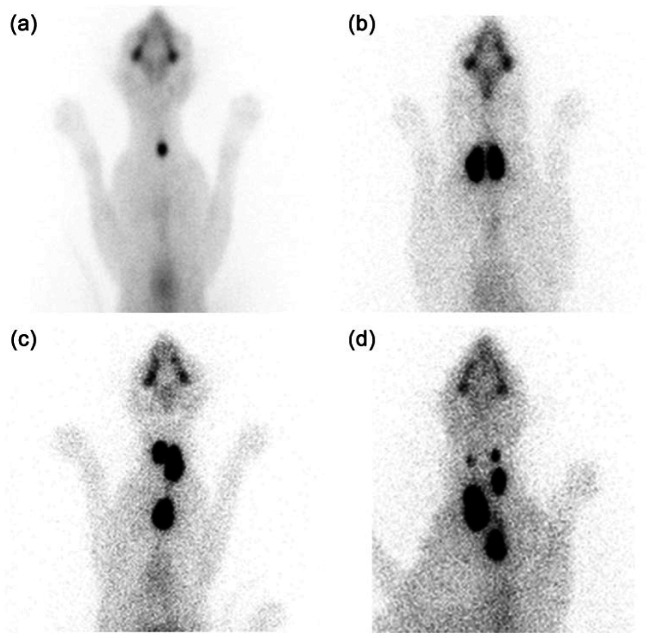
Methods: This was a cross-sectional study of 2096 cats with hyperthyroidism. Cats were divided into five groups based on time from diagnosis: ⩽1 year (n = 1773); >1-2 years (n = 169); >2-3 years (n = 88); >3-4 years (n = 35); and >4-6.1 years (n = 31). Methimazole, administered to 996 (47.5%) cats, was stopped at least 1 week prior to examination to allow for serum T4 testing. Each thyroid scintiscan was evaluated for pattern (unilateral, bilateral, multifocal), location (cervical, thoracic inlet, chest) and size (small, medium, large, huge) of the thyroid tumor, as well as features suggesting malignancy.
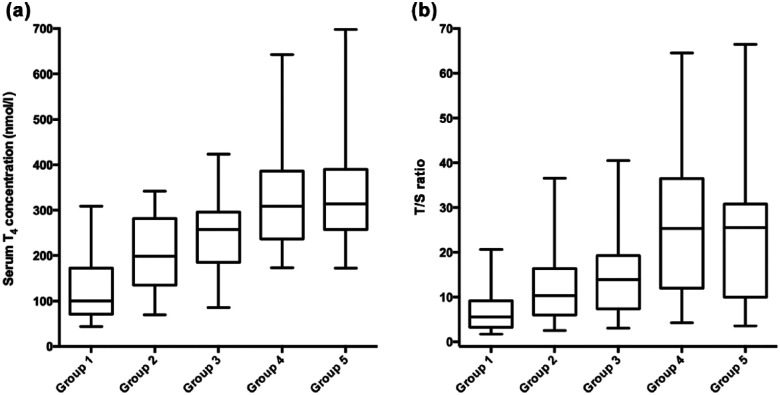
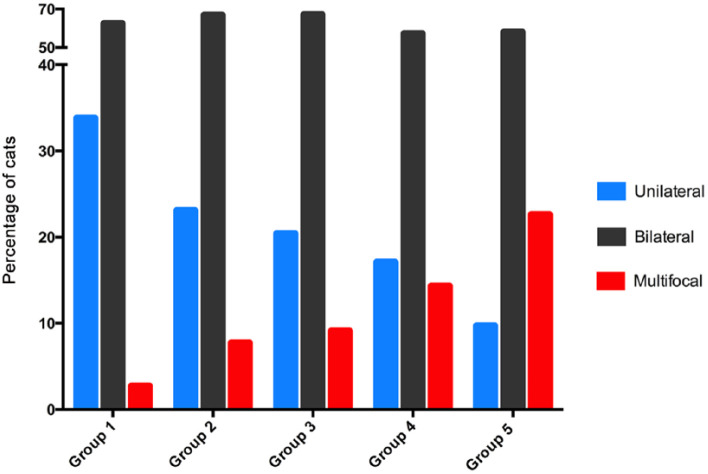
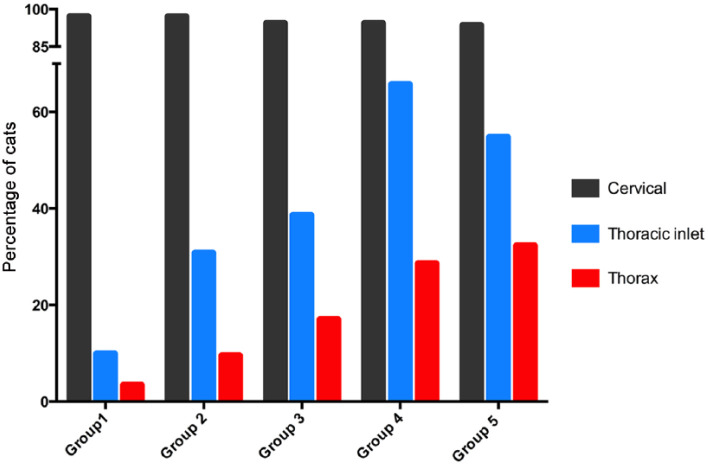
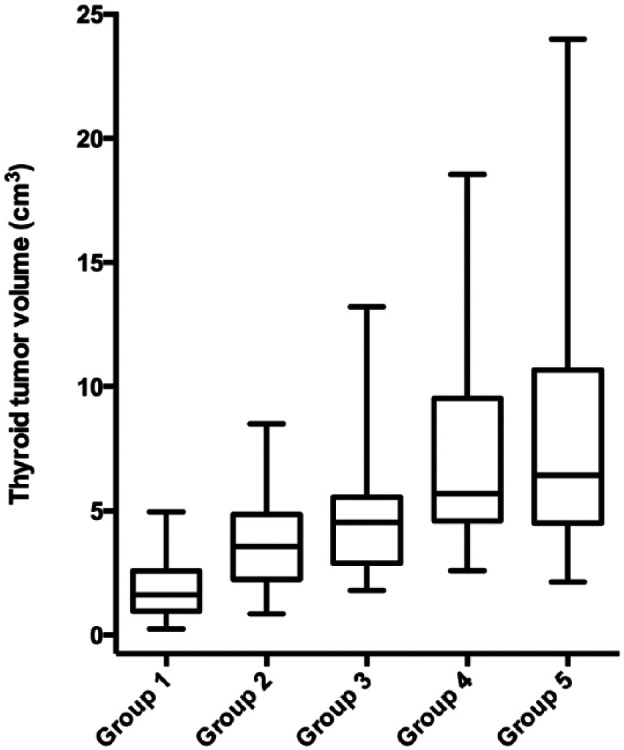
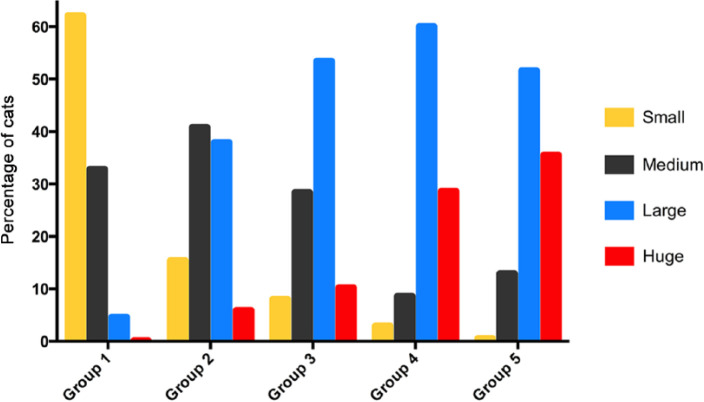
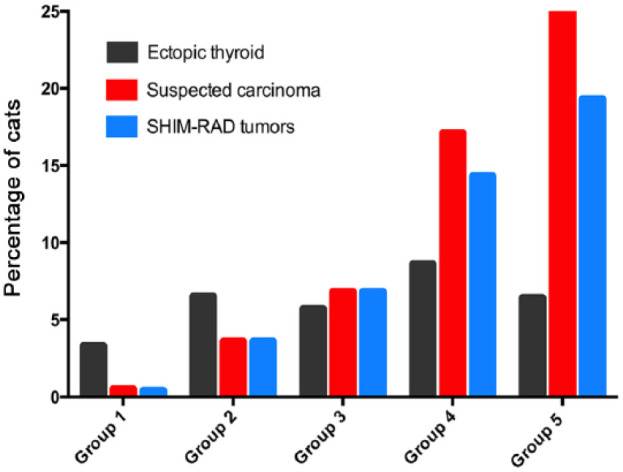
Results: Median serum T4 concentration increased with increasing disease duration from 100 nmol/l (⩽1 year) to 315 nmol/l (>4-6.1 years) (P <0.001). Prevalence of unilateral thyroid disease decreased, whereas multifocal disease (three or more tumor nodules) increased (P <0.001) with increasing disease duration. Median tumor volume in the five groups increased from 1.6 cm(3) (⩽1 year) to 6.4 cm(3) (>4-6.1 years). Prevalence of large (4-8 cm(3)) and huge (>8 cm(3)) thyroid tumors increased from 5.1% (⩽1 year) to 88.6% (>4-6.1 years), while the prevalence of intrathoracic tumor tissue increased from 3.4% (⩽1 year) to 32.3% (>4-6.1 years). Prevalence of suspected thyroid carcinoma (characterized by severe hyperthyroidism; huge, intrathoracic, multifocal tumors; refractory to methimazole treatment) increased with increasing disease duration from 0.4% (⩽1 year) to 19.3% (>4-6.1 years).
Conclusions and relevance: Our results indicate that the prevalence of severe hyperthyroidism, large thyroid tumors, multifocal disease, intrathoracic thyroid masses and suspected malignant disease all increase with disease duration in cats referred for radioiodine therapy.
© ISFM and AAFP 2015.
Conflict of interest statement
The authors do not have any potential conflicts of interest to declare.
Figures
References
-
- Baral R, Peterson ME. Thyroid gland disorders. In: Little SE. (ed). The cat: clinical medicine and management. Philadelphia, PA: Elsevier Saunders, 2012, pp 571–592.
-
- Mooney CT, Peterson ME. Feline hyperthyroidism. In: Mooney CT, Peterson ME. (eds). Manual of canine and feline endocrinology. 4th ed. Quedgeley: British Small Animal Veterinary Association, 2012, pp 199–203.
-
- Turrel JM, Feldman EC, Nelson RW, et al.. Thyroid carcinoma causing hyperthyroidism in cats: 14 cases (1981–1986). J Am Vet Med Assoc 1988; 193: 359–364. - PubMed
-
- Gerber H, Peter H, Ferguson DC, et al.. Etiopathology of feline toxic nodular goiter. Vet Clin North Am Small Anim Pract 1994; 24: 541–565. - PubMed
-
- Peterson ME, Broome MR. Thyroid scintigraphy findings in 2,096 cats with hyperthyroidism. Vet Radiol Ultrasound 2015; 56: 84–95. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
