

Triple-negative breast cancer in African-American women: disparities versus biology
- PMID: 25673085
- PMCID: PMC5470637
- DOI: 10.1038/nrc3896
Triple-negative breast cancer in African-American women: disparities versus biology
Abstract
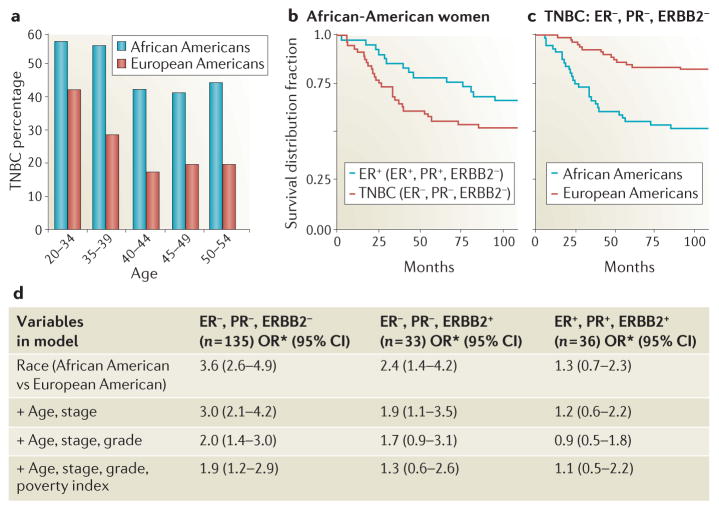
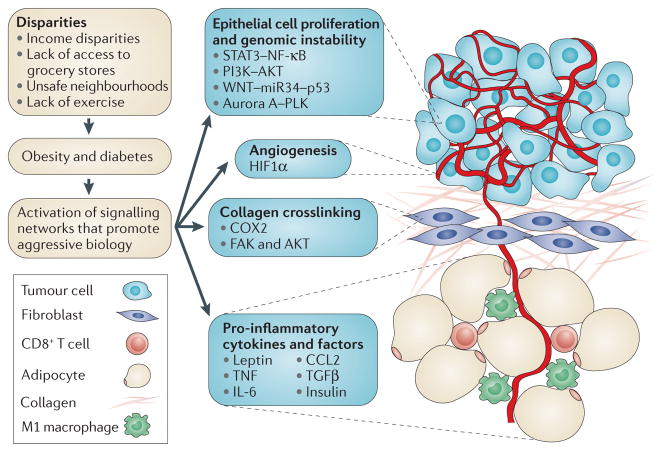
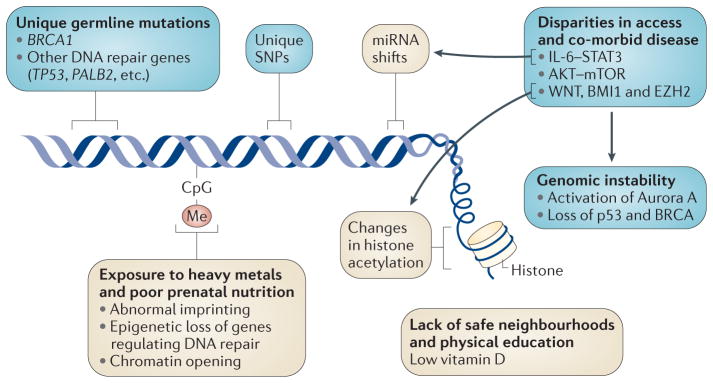
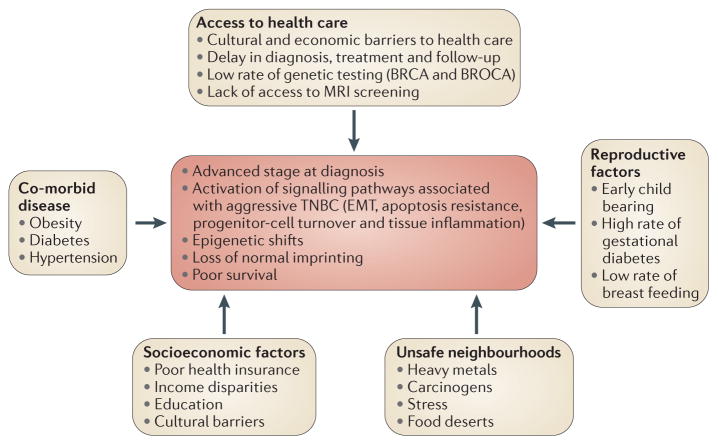
Triple-negative breast cancer (TNBC) is an aggressive breast cancer subtype that disproportionately affects BRCA1 mutation carriers and young women of African origin. There is evidence that African-American women with TNBC have worse clinical outcomes than women of European descent. However, it is unclear whether survival differences persist after adjusting for disparities in access to health-care treatment, co-morbid disease and income. It remains controversial whether TNBC in African-American women is a molecularly distinct disease or whether African-American women have a higher incidence of aggressive biology driven by disparities: there is evidence in support of both. Understanding the relative contributions of biology and disparities is essential for improving the poor survival rate of African-American women with TNBC.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363:1938–1948. - PubMed
-
- Carey LA, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295:2492–2502. - PubMed
-
- Lund MJ, et al. Race and triple negative threats to breast cancer survival: a population-based study in Atlanta, GA. Breast Cancer Res Treat. 2009;113:357–370. - PubMed
-
- Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer registry. Cancer. 2007;109:1721–1728. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
