

Candida colonization as a risk marker for invasive candidiasis in mixed medical-surgical intensive care units: development and evaluation of a simple, standard protocol
- PMID: 25673797
- PMCID: PMC4365204
- DOI: 10.1128/JCM.03239-14
Candida colonization as a risk marker for invasive candidiasis in mixed medical-surgical intensive care units: development and evaluation of a simple, standard protocol
Abstract
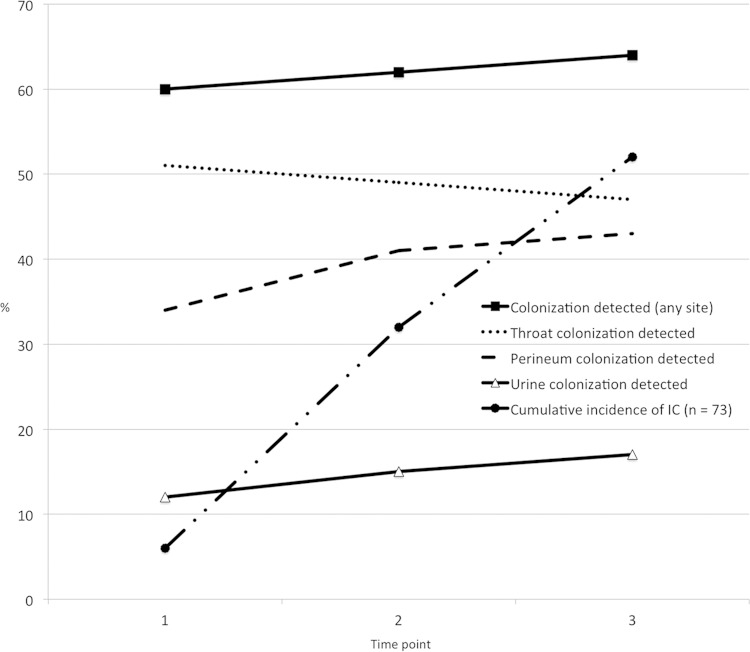
Colonization with Candida species is an independent risk factor for invasive candidiasis (IC), but the minimum and most practicable parameters for prediction of IC have not been optimized. We evaluated Candida colonization in a prospective cohort of 6,015 nonneutropenic, critically ill patients. Throat, perineum, and urine were sampled 72 h post-intensive care unit (ICU) admission and twice weekly until discharge or death. Specimens were cultured onto chromogenic agar, and a subset underwent molecular characterization. Sixty-three (86%) patients who developed IC were colonized prior to infection; 61 (97%) tested positive within the first two time points. The median time from colonization to IC was 7 days (range, 0 to 35). Colonization at any site was predictive of IC, with the risk of infection highest for urine colonization (relative risk [RR]=2.25) but with the sensitivity highest (98%) for throat and/or perineum colonization. Colonization of ≥2 sites and heavy colonization of ≥1 site were significant independent risk factors for IC (RR=2.25 and RR=3.7, respectively), increasing specificity to 71% to 74% but decreasing sensitivity to 48% to 58%. Molecular testing would have prompted a resistance-driven decision to switch from fluconazole treatment in only 11% of patients infected with C. glabrata, based upon species-level identification alone. Positive predictive values (PPVs) were low (2% to 4%) and negative predictive values (NPVs) high (99% to 100%) regardless of which parameters were applied. In the Australian ICU setting, culture of throat and perineum within the first two time points after ICU admission captures 84% (61/73 patients) of subsequent IC cases. These optimized parameters, in combination with clinical risk factors, should strengthen development of a setting-specific risk-predictive model for IC.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Leroy O, Gangneux JP, Montravers P, Mira JP, Gouin F, Sollet JP, Carlet J, Reynes J, Rosenheim M, Regnier B, Lortholary O. 2009. Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005–2006). Crit Care Med 37:1612–1618. doi: 10.1097/CCM.0b013e31819efac0. - DOI - PubMed
-
- Morrell M, Fraser VJ, Kollef MH. 2005. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 49:3640–3645. doi: 10.1128/AAC.49.9.3640-3645.2005. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
