

The care pathway for children with urticaria, angioedema, mastocytosis
- PMID: 25674297
- PMCID: PMC4313464
- DOI: 10.1186/s40413-014-0052-x
The care pathway for children with urticaria, angioedema, mastocytosis
Abstract
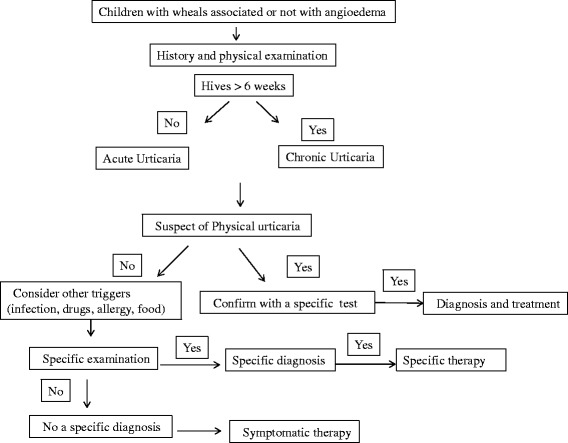
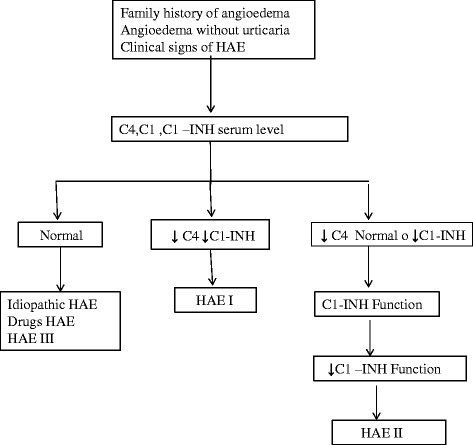
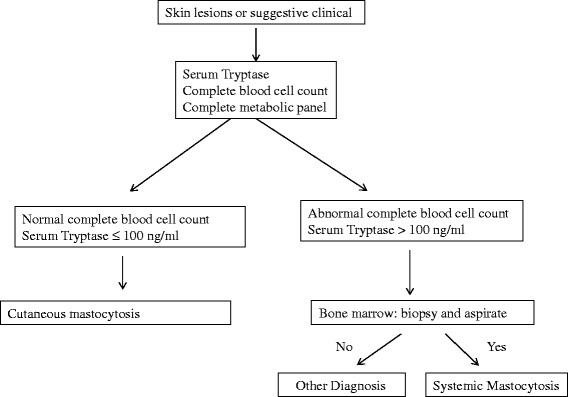
Cutaneous involvement characterized by urticarial lesions with or without angioedema and itch is commonly observed in routine medical practice. The clinical approach may still remain complex in real life, because several diseases may display similar cutaneous manifestations. Urticaria is a common disease, characterized by the sudden appearance of wheals, with/without angioedema. The term Chronic Urticaria (CU) encompasses a group of conditions with different underlying causes and different mechanisms, but sharing the clinical picture of recurring wheals and/or angioedema for at least 6 weeks. Hereditary Angioedema (HAE) is a rare disorder characterized by recurrent episodes of non-pruritic, non-pitting, subcutaneous or submucosal edema affecting the extremities, face, throat, trunk, genitalia, or bowel, that are referred as "attacks". HAE is an autosomal dominant disease caused by a deficiency of functional C1 inhibitor, due to a mutation in C1-INH gene (serping 1 gene) characterized by the clonal proliferation of mast cells, leading to their accumulation, and possibly mediator release, in one or more organs. In childhood there are two main forms of mastocytosis, the Systemic and the Cutaneous. The clinical features of skin lesions in urticaria, angioedema and mastocytosis may differ depending on the aetiologic factors, and the underlying pathophysiological mechanisms. The diagnostic process, as stepwise approach in routine clinical practice, is here reviewed for CU, HAE and mastocytosis, resulting in an integrated method for improved management of these cutaneous diseases. Taking into account that usually these conditions have also a relevant impact on the quality of life of children, affecting social activities and behavior, the availability of care pathways could be helpful in disentangle the diagnostic issue achieving the most cost-effective ratio.
Keywords: Angioedema; Children; Clinical practice; Diagnosis; Epidemiology; Itch; Management; Mastocytosis; Skin; Urticaria.
Figures
Similar articles
-
Diagnosis and treatment of hereditary angioedema.Panminerva Med. 2012 Sep;54(3):241-53. Panminerva Med. 2012. PMID: 22801442 Review.
-
The importance of recognizing and managing a rare form of angioedema: hereditary angioedema due to C1-inhibitor deficiency.Postgrad Med. 2021 Aug;133(6):639-650. doi: 10.1080/00325481.2021.1905364. Epub 2021 Jul 6. Postgrad Med. 2021. PMID: 33993830 Review.
-
Hereditary angioedema in childhood: an approach to management.Paediatr Drugs. 2010 Aug 1;12(4):257-68. doi: 10.2165/11532590-000000000-00000. Paediatr Drugs. 2010. PMID: 20593909 Review.
-
Angioedema Without Wheals: Challenges in Laboratorial Diagnosis.Front Immunol. 2021 Dec 8;12:785736. doi: 10.3389/fimmu.2021.785736. eCollection 2021. Front Immunol. 2021. PMID: 34956216 Free PMC article. Review.
-
Urticaria and angioedema.Med Clin North Am. 1992 Jul;76(4):805-40. doi: 10.1016/s0025-7125(16)30327-3. Med Clin North Am. 1992. PMID: 1614235 Review.
Cited by
-
Current approach to cutaneous mastocytosis in childhood.Turk Pediatri Ars. 2016 Sep 1;51(3):123-127. doi: 10.5152/TurkPediatriArs.2016.2418. eCollection 2016 Sep. Turk Pediatri Ars. 2016. PMID: 27738395 Free PMC article. Review.
-
Transient hypogammaglobulinaemia of infants in children with mastocytosis - strengthened indications for vaccinations.Cent Eur J Immunol. 2016;41(3):282-286. doi: 10.5114/ceji.2016.63128. Epub 2016 Oct 25. Cent Eur J Immunol. 2016. PMID: 27833446 Free PMC article.
-
Care for children with severe chronic skin diseases.Eur J Pediatr. 2019 Jul;178(7):1095-1103. doi: 10.1007/s00431-019-03366-z. Epub 2019 May 22. Eur J Pediatr. 2019. PMID: 31119437
-
Vitamin D in atopic dermatitis, chronic urticaria and allergic contact dermatitis.Expert Rev Clin Immunol. 2016 Aug;12(8):839-47. doi: 10.1586/1744666X.2016.1171143. Epub 2016 Apr 14. Expert Rev Clin Immunol. 2016. PMID: 27014952 Free PMC article. Review.
-
Mastocytosis: from a Molecular Point of View.Clin Rev Allergy Immunol. 2018 Jun;54(3):397-411. doi: 10.1007/s12016-017-8619-2. Clin Rev Allergy Immunol. 2018. PMID: 28725969 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
