

Clinical management of infertile men with nonobstructive azoospermia
- PMID: 25677138
- PMCID: PMC4430952
- DOI: 10.4103/1008-682X.148719
Clinical management of infertile men with nonobstructive azoospermia
Abstract
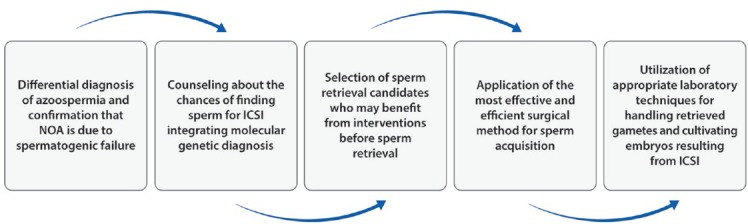
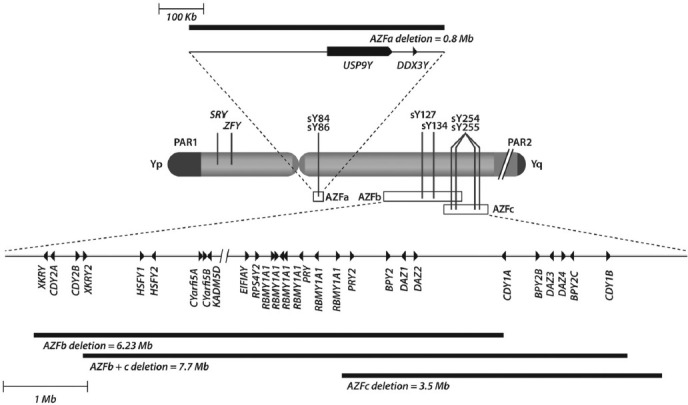
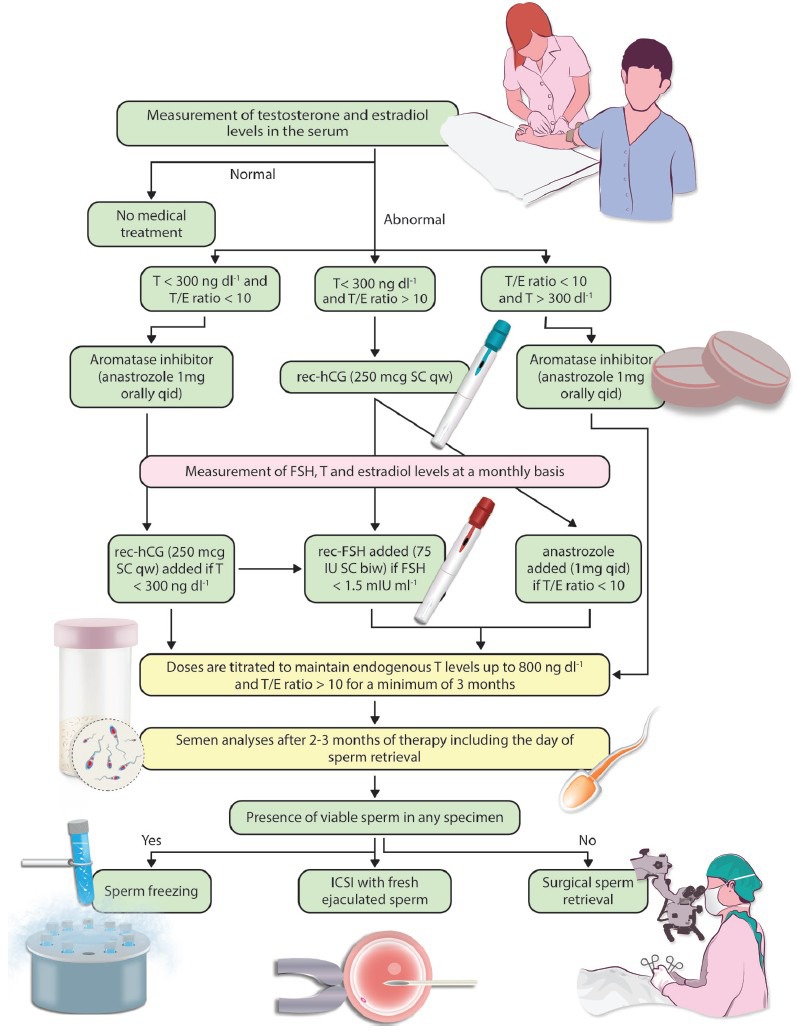
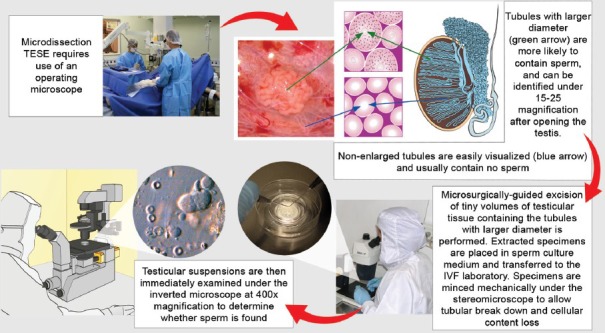
The clinical management of men with nonobstructive azoospermia (NOA) seeking fertility has been a challenge for andrologists, urologists, and reproductive medicine specialists alike. This review presents a personal perspective on the clinical management of NOA, including the lessons learned over 15 years dealing with this male infertility condition. A five-consecutive-step algorithm is proposed to manage such patients. First, a differential diagnosis of azoospermia is made to confirm/establish that NOA is due to spermatogenic failure. Second, genetic testing is carried out not only to detect the males in whom NOA is caused by microdeletions of the long arm of the Y chromosome, but also to counsel the affected patients about their chances of having success in sperm retrieval. Third, it is determined whether any intervention prior to a surgical retrieval attempt may be used to increase sperm production. Fourth, the most effective and efficient retrieval method is selected to search for testicular sperm. Lastly, state-of-art laboratory techniques are applied in the handling of retrieved gametes and cultivating the embryos resulting from sperm injections. A coordinated multidisciplinary effort is key to offer the best possible chance of achieving a biological offspring to males with NOA.
Figures
References
-
- Cooper TG, Hellenkemper B, Jonckheere J, Callewaert N, Grootenhuis AJ, et al. Azoospermia: virtual reality or possible to quantify? J Androl. 2006;27:483–90. - PubMed
-
- Silber SJ. Microsurgical TESE and the distribution of spermatogenesis in non-obstructive azoospermia. Hum Reprod. 2000;15:2278–84. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
