

Conservative interventions for preventing clinically detectable upper-limb lymphoedema in patients who are at risk of developing lymphoedema after breast cancer therapy
- PMID: 25677413
- PMCID: PMC10651942
- DOI: 10.1002/14651858.CD009765.pub2
Conservative interventions for preventing clinically detectable upper-limb lymphoedema in patients who are at risk of developing lymphoedema after breast cancer therapy
Abstract
Background: Breast cancer-related lymphoedema can be a debilitating long-term sequela of breast cancer treatment. Several studies have investigated the effectiveness of different treatment strategies to reduce the risk of breast cancer-related lymphoedema.
Objectives: To assess the effects of conservative (non-surgical and non-pharmacological) interventions for preventing clinically-detectable upper-limb lymphoedema after breast cancer treatment.
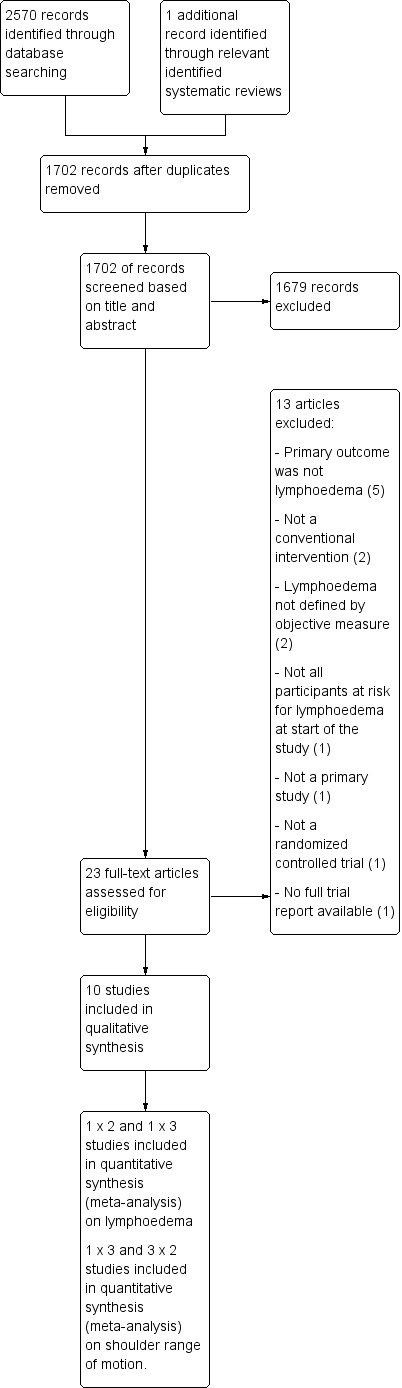
Search methods: We searched the Cochrane Breast Cancer Group's (CBCG) Specialised Register, CENTRAL, MEDLINE, EMBASE, CINAHL, PEDro, PsycINFO, and the World Health Organization (WHO) International Clinical Trials Registry Platform in May 2013. Reference lists of included trials and other systematic reviews were searched.
Selection criteria: Randomised controlled trials that reported lymphoedema as the primary outcome and compared any conservative intervention to either no intervention or to another conservative intervention.
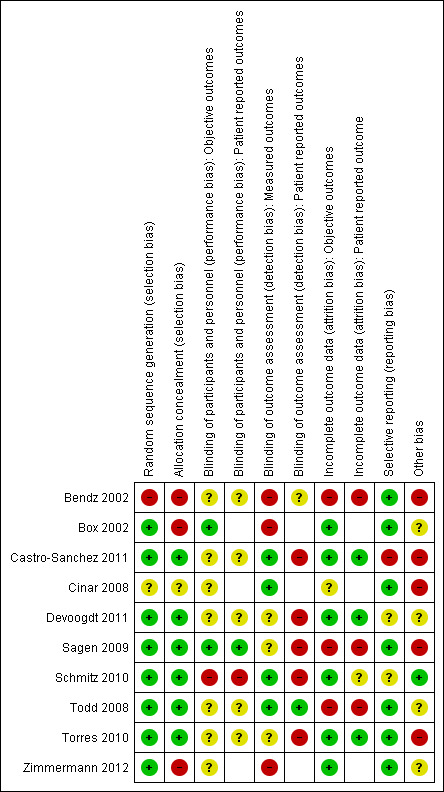
Data collection and analysis: Three authors independently assessed the risk of bias and extracted data. Outcome measures included lymphoedema, infection, range of motion of the shoulder, pain, psychosocial morbidity, level of functioning in activities of daily life (ADL), and health-related quality of life (HRQoL). Where possible, meta-analyses were performed. Risk ratio (RRs) or hazard ratio (HRs) were reported for dichotomous outcomes or lymphoedema incidence, and mean differences (MDs) for range of motion and patient-reported outcomes.
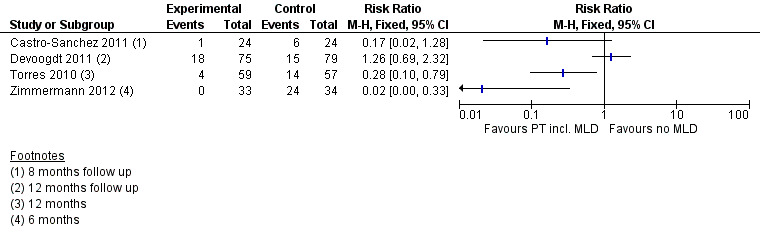
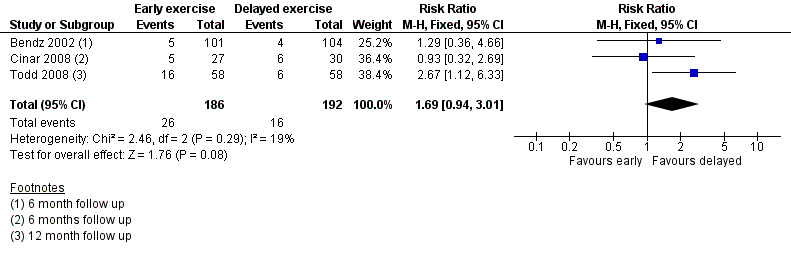
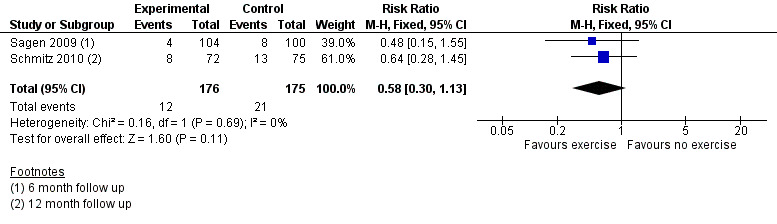
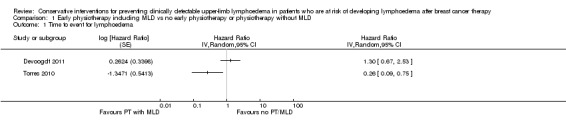
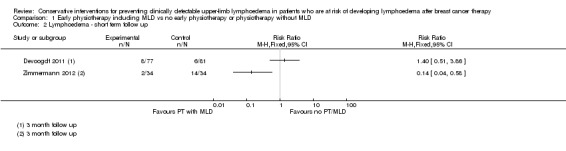
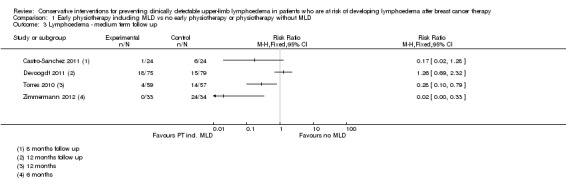
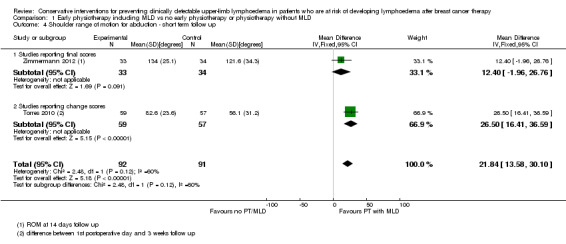
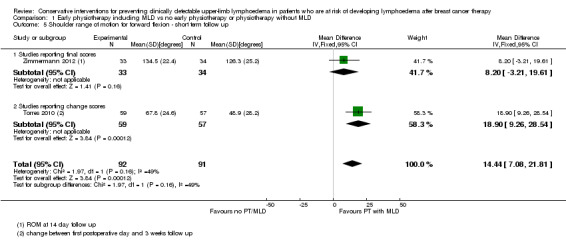
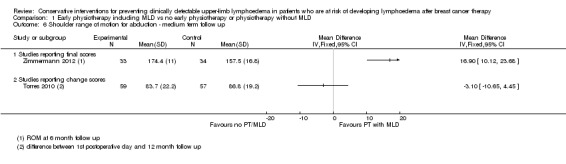
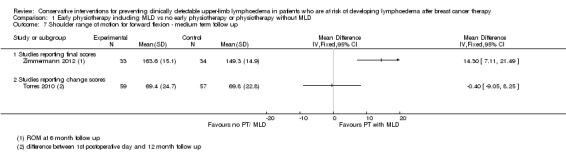
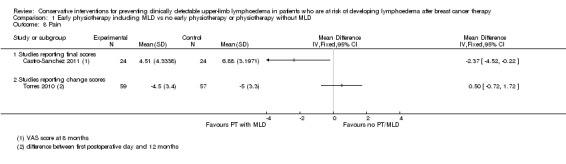
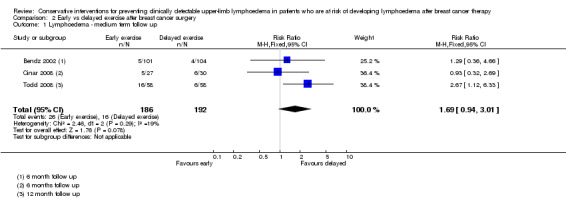
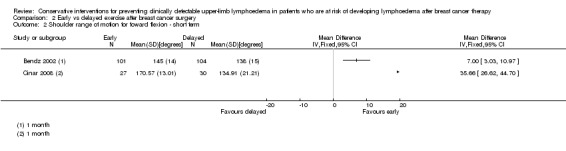
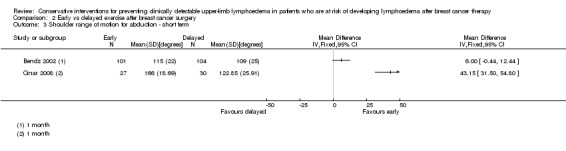
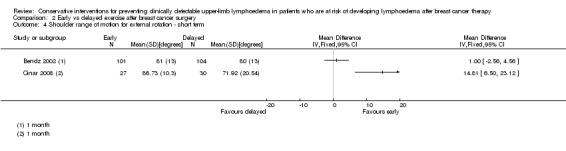
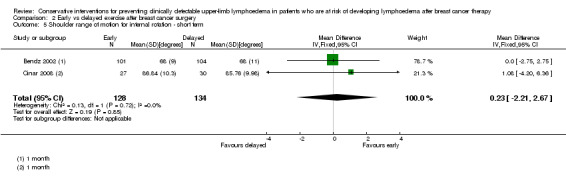
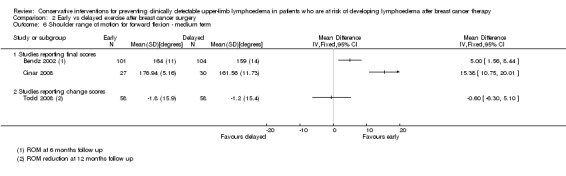
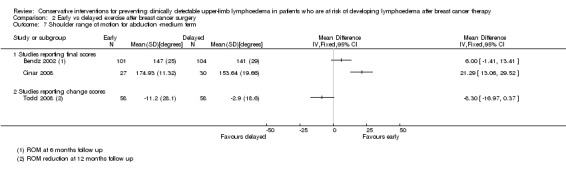
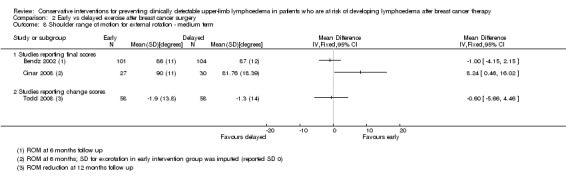
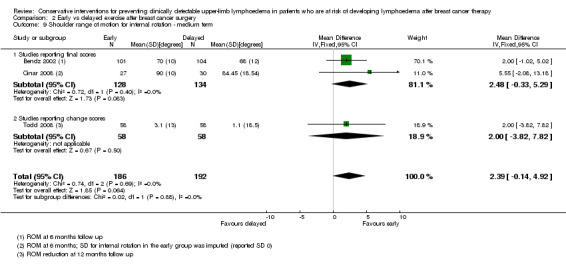
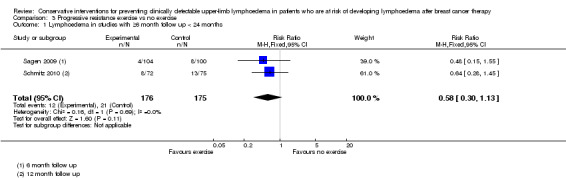
Main results: Ten trials involving 1205 participants were included. The duration of patient follow-up ranged from 2 days to 2 years after the intervention. Overall, the quality of the evidence generated by these trials was low, due to risk of bias in the included trials and inconsistency in the results. Manual lymph drainageIn total, four studies used manual lymph drainage (MLD) in combination with usual care or other interventions. In one study, lymphoedema incidence was lower in patients receiving MLD and usual care (consisting of standard education or exercise, or both) compared to usual care alone. A second study reported no difference in lymphoedema incidence when MLD was combined with physiotherapy and education compared to physiotherapy alone. Two other studies combining MLD with compression and scar massage or exercise observed a reduction in lymphoedema incidence compared to education only, although this was not significant in one of the studies. Two out of the four studies reported on shoulder mobility where MLD combined with exercise gave better shoulder mobility for lateral arm movement (shoulder abduction) and forward flexion in the first weeks after breast cancer surgery, compared to education only (mean difference for abduction 22°; 95% confidence interval (CI) 14 to 30; mean difference for forward flexion 14°; 95% CI 7 to 22). Two of the studies on MLD reported on pain, with inconsistent results. Results on HRQoL in two studies on MLD were also contradictory. Exercise: early versus delayed start of shoulder mobilising exercisesThree studies examined early versus late start of postoperative shoulder exercises. The pooled relative risk of lymphoedema after an early start of exercises was 1.69 (95% CI 0.94 to 3.01, 3 studies, 378 participants). Shoulder forward flexion was better at one and six months follow-up for participants who started early with mobilisation exercises compared to a delayed start (two studies), but no meta-analysis could be performed due to statistical heterogeneity. There was no difference in shoulder mobility or self-reported shoulder disability at 12 months follow-up (one study). One study evaluated HRQoL and reported difference at one year follow-up (mean difference 1.6 points, 95% CI -2.14 to 5.34, on the Trial Outcome Index of the FACT-B). Two studies collected data on wound drainage volumes and only one study reported higher wound drainage volumes in the early exercise group. Exercise: resistance trainingTwo studies compared progressive resistance training to restricted activity. Resistance training after breast cancer treatment did not increase the risk of developing lymphoedema (RR 0.58; 95% CI 0.30 to 1.13, two studies, 358 participants) provided that symptoms are monitored and treated immediately if they occur. One out of the two studies measured pain where participants in the resistance training group reported pain more often at three months and six months compared to the control group. One study reported HRQoL and found no significant difference between the groups. Patient education, monitoring and early interventionOne study investigated the effects of a comprehensive outpatient follow-up programme, consisting of patient education, exercise, monitoring of lymphoedema symptoms and early intervention for lymphoedema, compared to education alone. Lymphoedema incidence was lower in the comprehensive outpatient follow-up programme (at any time point) compared to education alone (65 people). Participants in the outpatient follow-up programme had a significantly faster recovery of shoulder abduction compared to the education alone group.
Authors' conclusions: Based on the current available evidence, we cannot draw firm conclusions about the effectiveness of interventions containing MLD. The evidence does not indicate a higher risk of lymphoedema when starting shoulder-mobilising exercises early after surgery compared to a delayed start (i.e. seven days after surgery). Shoulder mobility (that is, lateral arm movements and forward flexion) is better in the short term when starting shoulder exercises earlier compared to later. The evidence suggests that progressive resistance exercise therapy does not increase the risk of developing lymphoedema, provided that symptoms are closely monitored and adequately treated if they occur.Given the degree of heterogeneity encountered, limited precision, and the risk of bias across the included studies, the results of this review should be interpreted with caution.
Conflict of interest statement
The authors have no competing interests.
Figures

Update of
References
References to studies included in this review
Bendz 2002 {published data only}
-
- Bendz I, Fagevik Olsén M. Evaluation of immediate versus delayed shoulder exercises after breast cancer surgery including lymph node dissection ‐ A randomised controlled trial. The Breast 2002;11(3):241‐8. - PubMed
Box 2002 {published data only}
-
- Box RC, Reul‐Hirche HM, Bullock‐Saxton JE, Furnival CM. Physiotherapy after breast cancer surgery: results of a randomised controlled study to minimise lymphoedema. Breast Cancer Research and Treatment 2002;75(1):51‐64. - PubMed
-
- Box RC, Reul‐Hirche HM, Bullock‐Saxton JE, Furnival CM. Shoulder movement after breast cancer surgery: results of a randomised controlled study of postoperative physiotherapy. Breast Cancer Research and Treatment 2002;75(1):35‐50. - PubMed
Castro‐Sanchez 2011 {published data only}
-
- Castro‐Sánchez AM, Moreno‐Lorenzo C, Matarán‐Peñarrocha GA, Aguilar‐Ferrándiz ME, Almagro‐Céspedes I, Anaya‐Ojeda J. Preventing lymphoedema after breast cancer surgery by elastic restraint orthotic and manual lymphatic drainage: a randomized clinical trial. Medicina Clinica 2010;137(5):204‐7. - PubMed
Cinar 2008 {published data only}
-
- Cinar N, Seckin U, Keskin D, Bodur H, Bozkurt B, Cengiz O. The effectiveness of early rehabilitation in patients with modified radical mastectomy. Cancer nursing 2008;31(2):160‐5. [PUBMED: 18490892] - PubMed
Devoogdt 2011 {published data only}
Sagen 2009 {published data only}
-
- Sagen A, Kåresen R, Risberg MA. Physical activity for the affected limb and arm lymphedema after breast cancer surgery. A prospective, randomized controlled trial with two years follow‐up. Acta Oncologica 2009;48:1102‐10. - PubMed
Schmitz 2010 {published data only}
-
- Schmitz KH, Ahmed RL, Troxel AB, Cheville A, Lewis‐Grant L, Smith R, et al. Weight lifting for women at risk for breast cancer‐related lymphedema: a randomized trial. JAMA 2010;304(24):2699‐705. - PubMed
-
- Speck RM, Gross CR, Hormes JM, Ahmed RL, Lytle LA, Hwang WT, et al. Changes in the Body Image and Relationship Scale following a one‐year strength training trial for breast cancer survivors with or at risk for lymphedema. Breast Cancer Research and Treatment 2010;121(2):421‐30. - PubMed
Todd 2008 {published data only}
-
- Todd J, Scally A, Dodwell D, Horgan K, Topping A. A randomised controlled trial of two programmes of shoulder exercise following axillary node dissection for invasive breast cancer. Physiotherapy 2008;94:265‐73.
Torres 2010 {published data only}
Zimmermann 2012 {published data only}
-
- Zimmermann A, Szklarska A, Lipowicz A, Woźniewski M. Influence of manual lymph drainage on shoulder range of motion after breast cancer surgery; a randomized controlled trial [Einfluss der manuellen Lymphdrainage auf die Schulterbeweglichkeit nach Brustkrebsoperation Eine randomisierte kontrollierte klinische Studie]. PT_Zeitschrift für Physiotherapeuten 2009;7(61):602‐610.
-
- Zimmermann A, Woźniewski M, Szklarska A, Lipowicz A, Szuba A. Efficacy of manual lymphatic drainage in preventing secondary lymphedema after breast cancer surgery. Lymphology 2012;45(3):103‐12. - PubMed
References to studies excluded from this review
Ahmed 2006 {published data only}
-
- Ahmed RL, Thomas W, Yee D, Schmitz KH. Randomized controlled trial of weight training and lymphedema in breast cancer survivors. Journal of Clinical Oncology 2006;24(18):2765‐72. - PubMed
Anderson 2012 {published data only}
Boccardo 2009 {published data only}
-
- Boccardo FM, Ansaldi F, Bellini C, Accogli S, Taddei G, Murdaca G, et al. Prospective evaluation of a prevention protocol for lymphedema following surgery for breast cancer. Lymphology 2009;1(42):1‐9. - PubMed
Box 2009 {published data only}
-
- Box R. Restriction of the range of arm elevation exercises for one week after surgery for breast cancer can reduce the incidence of lymphoedema. Australian Journal of Physiotherapy 2009;55(1):64‐6. - PubMed
Campisi 2002 {published data only}
-
- Campisi C, Boccardo F, Zilli A, Maccio A, Napoli F, Ferreira Azevedo W Jr, et al. Lymphedema secondary to breast cancer treatment: possibility of diagnostic and therapeutic prevention. Annali Italiani di Chirurgia 2002;73(5):493‐8. - PubMed
Chandrakaladharan 2009 {published data only}
-
- Chandrakaladharan BS, Paul MJ, Nair A. Randomized control trial to evaluate the influence of class II compression stockings in preventing the development of lymphoedema in breast carcinoma patients. Annals of Oncology. 2009; Vol. Conference: IMPAKT Breast Cancer Conference Brussels Belgium 2009, issue conference publication ii69.
de Rezende 2006 {published data only}
-
- Rezende LF, Franco RL, Rezende MF, Beletti PO, Morais SS, Gurgel MS. Two exercise schemes in postoperative breast cancer: comparison of effects on shoulder movement and lymphatic disturbance. Tumori 2006;92(1):55‐61. - PubMed
Hayes 2012 {published data only}
-
- Hayes SC, Rye S, Disipio T, Yates P, Bashford J, Pyke C, et al. Exercise for health: a randomized, controlled trial evaluating the impact of a pragmatic, translational exercise intervention on the quality of life, function and treatment‐related side effects following breast cancer. Breast Cancer Research and Treatment 2012;137(1):175‐86. - PubMed
Le‐Vu 1997 {published data only}
-
- Le‐Vu B, Guillaume MHB. Efficacy of massage and mobilization of the upper limb after surgical treatment of breast cancer. Bulletin du Cancer 1997;84(10):957‐61. - PubMed
Oliveira 2009 {published data only}
-
- Oliveira MMF, Gurgel MSC, Miranda MS, Okubo MA, Feijó LFA, Souza GA. Efficacy of shoulder exercises on locoregional complications in women undergoing radiotherapy for breast cancer: clinical trial. Revista Brasileira de Fisioterapia [Brazilian Journal of Physical Therapy] 2009;13(2):136‐43.
Sarri 2010 {published data only}
Sisman 2012 {published data only}
-
- Sisman H, Sahin B, Duman BB, Tanriverdi G. Nurse‐assisted education and exercise decrease the prevalence and morbidity of lymphedema following breast cancer surgery. Journal of B.U.ON. 2012;17(3):565‐9. - PubMed
Wang 2005 {published data only}
-
- Wang BG, Yuan XY, Wang QT, Luang XD, Wang CP, Jia AL, et al. (2005) [Functional rehabilitation gymnastics for the edema of upper limbs and the activity of shoulder joint in postoperative patients with breast cancer]. " Zhongguo Linchuang Kangfu [Chinese Journal of Clinical Rehabilitation] 2005;9(30):16‐9.
References to ongoing studies
Ben Selvan 2008 {published data only}
-
- The influence of prophylactic application of the class 2 upper limb stockings in carcinoma breast patients in reducing the incidence of Breast cancer related lymph edema. Ongoing study Registered on 27‐11‐2008.
Pain 2012 {published data only}
-
- Prevention of breast cancer‐related lymphoedema following axillary lymph node clearance.. Ongoing study 1‐10‐2011.
Additional references
Altman 1996
Brennan 1992
-
- Brennan MJ. Lymphedema following the surgical treatment of breast cancer: a review of pathophysiology and treatment. Journal of Pain and Symptom Management 1992;7:110‐6. - PubMed
Chan 2010
-
- Chan DN, Lui LY, So WK. Effectiveness of exercise programmes on shoulder mobility and lymphoedema after axillary lymph node dissection for breast cancer: systematic review. Journal of advanced nursing 2010;66(9):1902‐14. [PUBMED: 20626480] - PubMed
Clark 2005
-
- Clark B, Sitzia J, Harlow W. Incidence and risk of arm oedema following treatment for breast cancer: a three‐year follow‐up study. QJM: Monthly Journal of the Association of Physicians 2005;98(5):343‐8. - PubMed
Cormier 2010
-
- Cormier JN, Askew RL, Mungovan KS, Xing Y, Ross MI, Armer JM. Lymphedema beyond breast cancer: a systematic review and meta‐analysis of cancer‐related secondary lymphedema. Cancer 2010;116:5138‐49. - PubMed
DerSimonian 1986
-
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. - PubMed
Devoogdt 2010
-
- Devoogdt N, Kampen M, Geraerts I, Coremans T, Christiaens MR. Different physical treatment modalities for lymphoedema developing after axillary lymph node dissection for breast cancer: a review. European journal of obstetrics, gynecology, and reproductive biology 2010;149(1):3‐9. [PUBMED: 20018422] - PubMed
DiSipio 2013
-
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta‐analysis. The lancet oncology 2013;14(6):500‐15. [PUBMED: 23540561] - PubMed
Duets
-
- NHS. NHS Database of Uncertainties about the Effects of Treatments (DUETS):. http://www.library.nhs.uk/DUETs/ViewResource.aspx?resID=302437 accessed June 2011.
Engel 2003
-
- Engel J, Kerr J, Schlesinger‐Raab A, Eckel R, Sauer H, Holzel D. Predictors of quality of life of breast cancer patients. Acta Oncologica 2003;42:710‐8. - PubMed
Ewertz 2011
-
- Ewertz M, Jensen AB. Late effects of breast cancer treatment and potentials for rehabilitation. Acta Oncologica 2011;50(2):187‐93. - PubMed
Fu 2010
-
- Fu MR, Chen CM, Haber J, Guth AA, Axelrod D. The effect of providing information about lymphedema on the cognitive and symptom outcomes of breast cancer survivors. Annals of surgical oncology 2010;17(7):1847‐53. [PUBMED: 20140528] - PubMed
Globocan 2008
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10. Available from: http://globocan.iarc.fr 2010.
Goldberg 2010
-
- Goldberg JI, Wiechmann LI, Riedel ER, Morrow M, Zee KJ. Morbidity of sentinel node biopsy in breast cancer: the relationship between the number of excised lymph nodes and lymphedema. Annals of Surgical Oncology 2010;17:3278‐86. - PubMed
Hayes 2008
-
- Hayes SC, Janda M, Cornish B, Battistutta D, Newman B. Lymphedema after breast cancer: incidence, risk factors, and effect on upper body function. Journal of Clinical Oncology 2008;26:3536‐42. - PubMed
Helyer 2010
-
- Helyer LK, Varnic M, Le LW, Leong W, McCready D. Obesity is a risk factor for developing postoperative lymphedema in breast cancer patients. Breast Journal 2010;16:48‐54. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kwan 2010
Lane 2007
-
- Lane KN, Dolan LB, Worsley D, McKenzie DC. Upper extremity lymphatic function at rest and during exercise in breast cancer survivors with and without lymphedema compared with healthy controls. Journal of Applied Physiology 2007;103:917‐25. - PubMed
Lee 2009
-
- Lee TS, Kilbreath SL, Sullivan G, Refshauge KM, Beith JM, Harris LM. Factors that affect intention to avoid strenuous arm activity after breast cancer surgery. Oncology Nursing Forum 2009;36:454‐62. - PubMed
Mantel 1959
-
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the National Cancer Institute 1959;22(4):719‐48. - PubMed
McNeely 2010
Meeske 2008
-
- Meeske KA, Sullivan‐Halley J, Smith AW, McTiernan A, Baumgartner KB, Harlan LC, et al. Risk factors for arm lymphedema following breast cancer diagnosis in Black women and White women. Breast Cancer Research and Treatment 2008;113:383‐91. - PubMed
Norman 2010
Park 2008
-
- Park JH, Lee WH, Chung HS. Incidence and risk factors of breast cancer lymphoedema. Journal of Clinical Nursing 2008;17(11):1450‐9. - PubMed
Parmar 1998
-
- Parmar MKB, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815‐34. - PubMed
Paskett 2007
Petrek 1998
-
- Petrek JA, Heelan MC. Incidence of breast carcinoma‐related lymphedema. American Cancer Society Lymphedema Workshop. Cancer 1998;83 Suppl(12):2776‐81. - PubMed
Preston 2008
R Statistical Package [Computer program]
-
- R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. Version 3.0.0. http://www.r‐project.org/, 2013.
RevMan 5 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Ridner 2011
Round 2006
-
- Round T, Hayes SC, Newman B. How do recovery advice and behavioural characteristics influence upper‐body function and quality of life among women 6 months after breast cancer diagnosis?. Supportive care in cancer: official journal of the Multinational Association of Supportive Care in Cancer 2006;14(1):22‐9. [PUBMED: 16012817] - PubMed
Schulz 2010
Shih 2009
-
- Shih YC, Xu Y, Cormier JN, Giordano S, Ridner SH, Buchholz TA, et al. Incidence, treatment costs, and complications of lymphedema after breast cancer among women of working age: a 2‐year follow‐up study. Journal of Clinical Oncology 2009;27:2007‐14. - PubMed
Stout 2008
-
- Stout Gergich NL, Pfalzer LA, McGarvey C, Springer B, Gerber LH, Soballe P. Preoperative assessment enables the early diagnosis and successful treatment of lymphedema. Cancer 2008;112:2809‐19. - PubMed
Tsai 2009a
-
- Tsai RJ, Dennis LK, Lynch CF, Snetselaar LG, Zamba GK, Scott‐Conner C. The risk of developing arm lymphedema among breast cancer survivors: a meta‐analysis of treatment factors. Annals of Surgical Oncology 2009;16:1959‐72. - PubMed
Tsai 2009b
-
- Tsai HJ, Hung HC, Yang JL, Huang CS, Tsauo JY. Could Kinesio tape replace the bandage in decongestive lymphatic therapy for breast‐cancer‐related lymphedema? A pilot study. Annals of Surgical Oncology 2009;16:1959‐72. - PubMed
Vassard 2010
-
- Vassard D, Olsen MH, Zinckernagel L, Vibe‐Petersen J, Dalton SO, Johansen C. Psychological consequences of lymphoedema associated with breast cancer: A prospective cohort study. European Journal of Cancer 2010;46:3211‐8. - PubMed
Wood 2008
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous