

Building Equity Improvement into Quality Improvement: Reducing Socioeconomic Disparities in Colorectal Cancer Screening as Part of Population Health Management
- PMID: 25678378
- PMCID: PMC4471039
- DOI: 10.1007/s11606-015-3227-4
Building Equity Improvement into Quality Improvement: Reducing Socioeconomic Disparities in Colorectal Cancer Screening as Part of Population Health Management
Abstract
Background: Improving colorectal cancer (CRC) screening rates for patients from socioeconomically disadvantaged backgrounds is a recognized public health priority.
Objective: Our aim was to determine if implementation of a system-wide screening intervention could reduce disparities in the setting of improved overall screening rates.
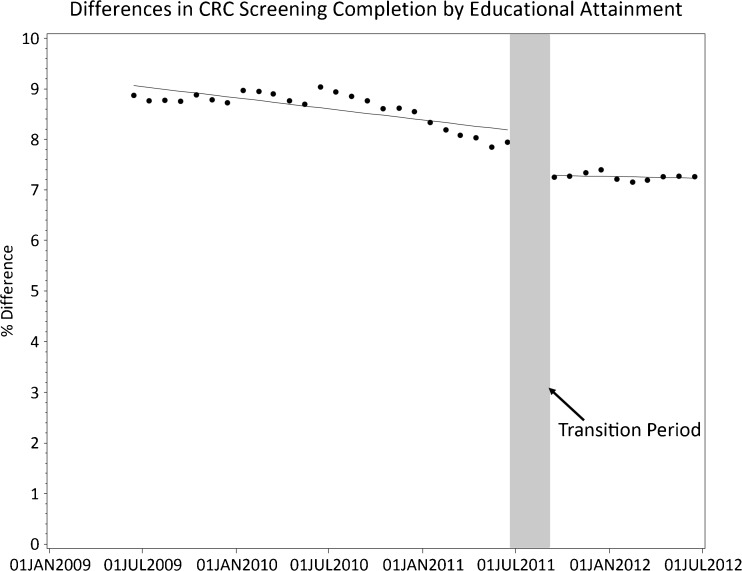
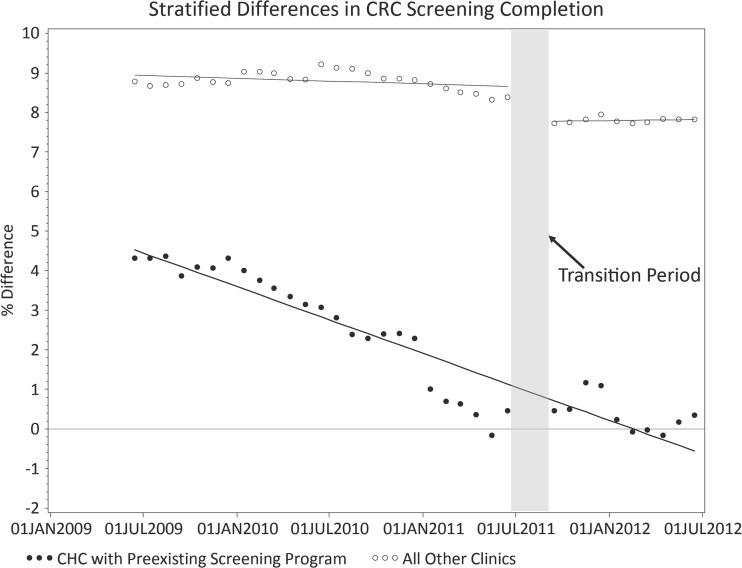
Design: This was an interrupted time series (ITS) analysis before and after a population management intervention.
Participants: Patients eligible for CRC screening (age 52-75 years without prior total colectomy) in an 18-practice research network from 15 June 2009 to 15 June 2012 participated in the study.
Intervention: The Technology for Optimizing Population Care (TopCare) intervention electronically identified patients overdue for screening and facilitated contact by letter or telephone scheduler, with or without physician involvement. Patients identified by algorithm as high risk for non-completion entered into intensive patient navigation.
Main measures: Patients were dichotomized as ≤ high school diploma (≤ HS), an indicator of socioeconomic disadvantage, vs. >HS diploma (> HS). The monthly disparity between ≤ HS and > HS with regard to CRC screening completion was examined.
Key results: At baseline, 72% of 47,447 eligible patients had completed screening, compared with 75% of 51,442 eligible patients at the end of follow-up (p < 0.001). CRC screening completion was lower in ≤ HS vs. >HS patients in June 2009 (65.7% vs. 74.5%, p < 0.001) and remained lower in June 2012 (69.4% vs. 76.7%, p < 0.001). In the ITS analysis, which accounts for secular trends, TopCare was associated with a significant decrease in the CRC screening disparity (0.7%, p < 0.001). The effect of TopCare represents approximately 99 additional ≤ HS patients screened above prevailing trends, or 26 life-years gained had these patients remained unscreened.
Conclusions: A multifaceted population management intervention sensitive to the needs of vulnerable patients modestly narrowed disparities in CRC screening, while also increasing overall screening rates. Embedding interventions for vulnerable patients within larger population management systems represents an effective approach to increasing overall quality of care while also decreasing disparities.
Figures
Comment in
-
Capsule Commentary on Berkowitz et al., Building Equity Improvement into Quality Improvement: Reducing Socioeconomic Disparities in Colorectal Cancer Screening as Part of Population Health Management.J Gen Intern Med. 2015 Jul;30(7):1001. doi: 10.1007/s11606-015-3244-3. J Gen Intern Med. 2015. PMID: 25722092 Free PMC article. No abstract available.
References
-
- U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2010 Incidence and Mortality Web-based Report. . U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute, Atlanta. 2013. www.cdc.gov/uscs. Accessed 28 January 2015.
-
- U.S. Preventive Services Task Force. Screening for Colorectal Cancer: U.S. Preventive Services Task Force Recommendation Statement. AHRQ Publication 08-05124-EF-3 2008. http://www.uspreventiveservicestaskforce.org/uspstf08/colocancer/colors.htm. Accessed 28 January 2015.
-
- Agency for Healthcare Research and Quality. National Healthcare Quality & Disparities Reports. . Rockville, MD. 2014. http://www.ahrq.gov/research/findings/nhqrdr/index.html. Accessed 28 January 2015.
-
- Steele CB, Rim SH, Joseph DA, King JB, Seeff LC. Colorectal cancer incidence and screening - United States, 2008 and 2010. MMWR Surveill Summ. 2013;62(3):53–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
