

Imaging appearance of dextranomer/hyaluronic acid copolymer implant injections for treatment of velopharyngeal insufficiency
- PMID: 25678484
- PMCID: PMC8013007
- DOI: 10.3174/ajnr.A4246
Imaging appearance of dextranomer/hyaluronic acid copolymer implant injections for treatment of velopharyngeal insufficiency
Abstract
Background and purpose: Dextranomer/hyaluronic acid copolymer implants are used in treating velopharyngeal insufficiency. These posterior nasopharyngeal implants can be mistaken for pathologic conditions such as retropharyngeal abscess on imaging. We studied the imaging appearance of dextranomer/hyaluronic acid copolymer implants in patients treated for velopharyngeal insufficiency.
Materials and methods: A consecutive series of patients with velopharyngeal insufficiency treated with dextranomer/hyaluronic acid copolymer were included in this study. Data on patient characteristics and volume of dextranomer/hyaluronic acid copolymer injected were obtained. Postoperative imaging characteristics on plain radiography, CT, and MR imaging were assessed. The imaging appearance of postoperative complications was determined.
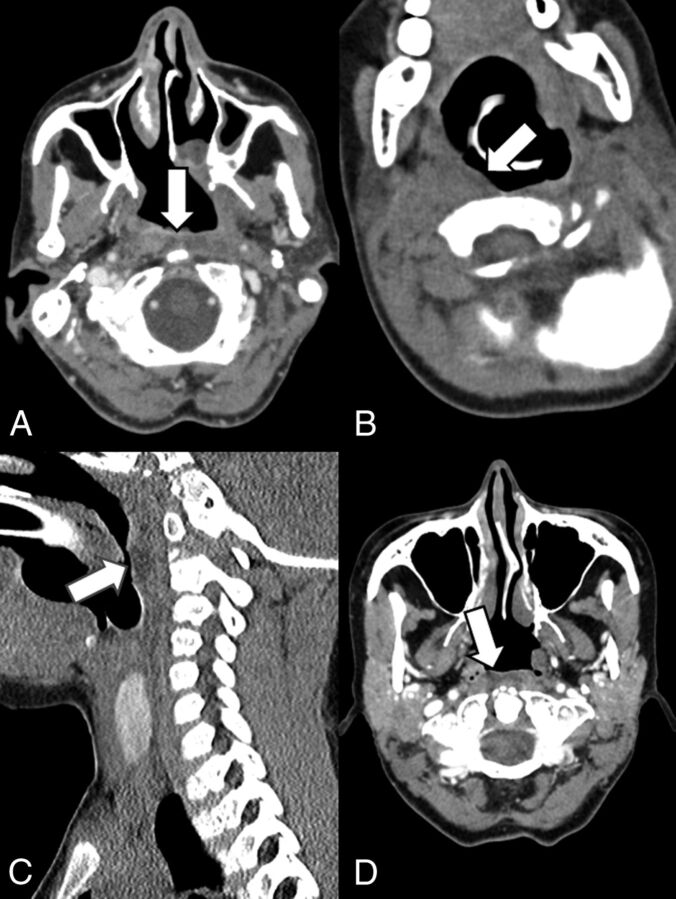
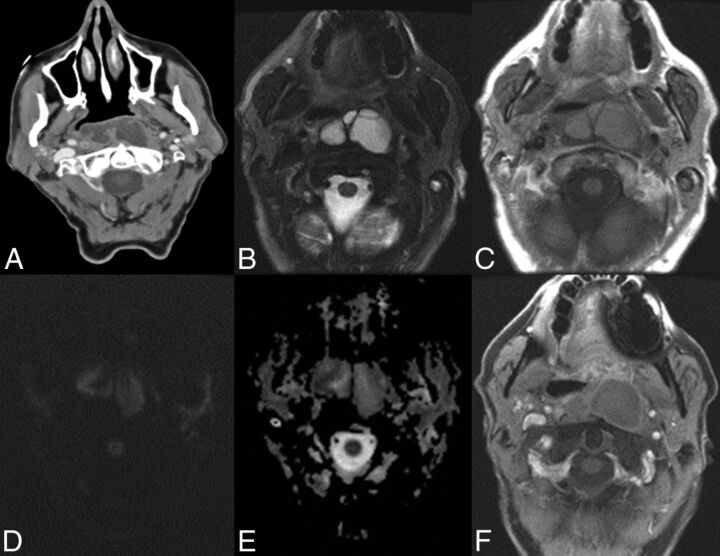
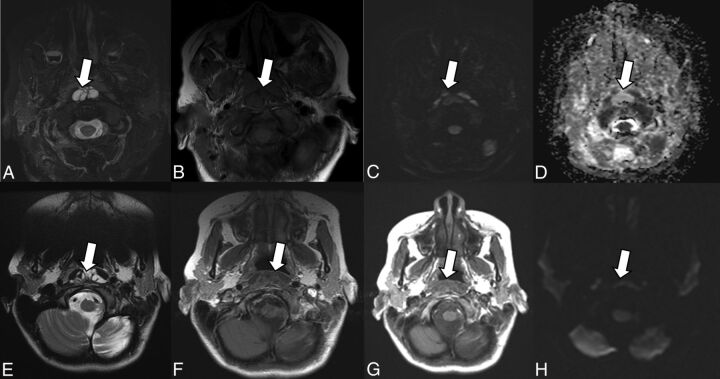
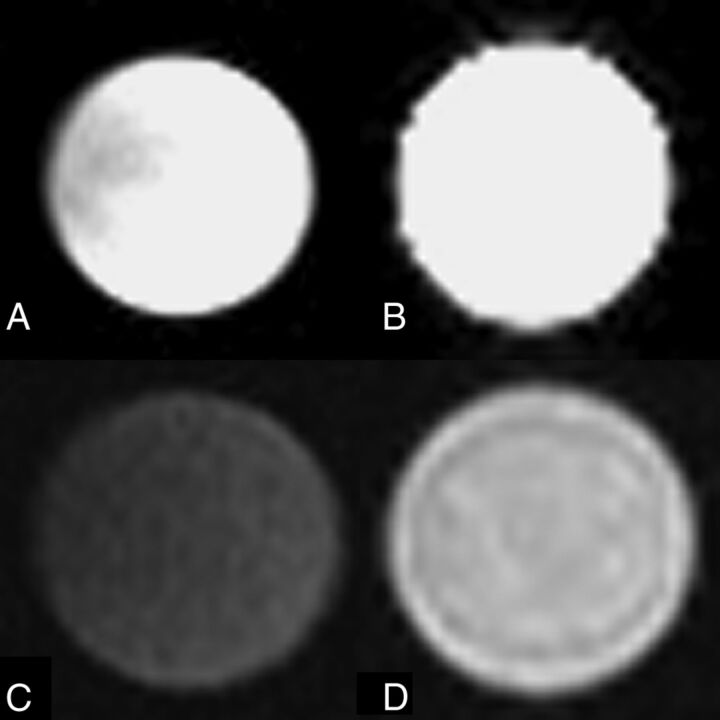
Results: Sixteen patients were included in this study. Seven patients underwent postoperative plain radiographs, 5 patients underwent CT, and 9 patients underwent MR imaging. Plain radiographs demonstrated soft-tissue swelling in the retropharyngeal space, which resolved at 1 month. On CT, dextranomer/hyaluronic acid copolymer implants appeared as bilateral nasopharyngeal soft-tissue masses isoattenuated to hypoattenuated relative to muscle in 80% (4/5) of patients. On MR imaging, dextranomer/hyaluronic acid copolymer implants appeared as bilateral nasopharyngeal soft-tissue masses that were isointense to muscle on T1 (8/9, 88.9%) and hyperintense to muscle on T2 (8/9, 88.9%) and demonstrated no restricted diffusion (4/4, 100.0%) or peripheral enhancement (7/7, 100.0%).
Conclusions: The normal postoperative findings of posterior nasopharyngeal dextranomer/hyaluronic acid copolymer injection on MR imaging is characterized by the presence of bilateral nasopharyngeal soft-tissue masses that are isointense to muscle on T1 and hyperintense on T2, with no restricted diffusion or peripheral enhancement. Velopharyngeal dextranomer/hyaluronic acid copolymer implants are iso- to hypoattenuated to muscle on CT and are not visible radiographically once associated implantation-related swelling has resolved.
© 2015 by American Journal of Neuroradiology.
Figures

References
-
- Brigger MT, Ashland JE, Hartnick CJ. Injection pharyngoplasty with calcium hydroxylapatite for velopharyngeal insufficiency: patient selection and technique. Arch Otolaryngol Head Neck Surg 2010;136:666–70 - PubMed
-
- Bluestone CD, Musgrave RH, McWilliams BJ, et al. . Teflon injection pharyngoplasty. Cleft Palate J 1968;5:19–22 - PubMed
-
- Cao Y, Ma T, Wu D, et al. . Autologous fat injection combined with palatoplasty and pharyngoplasty for velopharyngeal insufficiency and cleft palate: preliminary experience. Otolaryngol Head Neck Surg 2013;149:284–91 - PubMed
-
- Hagerty RF, Hill MJ. Cartilage pharyngoplasty in cleft palate patients. Surg Gynecol Obstet 1961;112:350–56 - PubMed
-
- Lando RL. Transplant of cadaveric cartilage into the posterior pharyngeal wall in treatment of cleft palate [article in undetermined language]. Stomatologiia (Mosk) 1950;4:38–39 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical