

Induction of T-cell Immunity Overcomes Complete Resistance to PD-1 and CTLA-4 Blockade and Improves Survival in Pancreatic Carcinoma
- PMID: 25678581
- PMCID: PMC4390506
- DOI: 10.1158/2326-6066.CIR-14-0215
Induction of T-cell Immunity Overcomes Complete Resistance to PD-1 and CTLA-4 Blockade and Improves Survival in Pancreatic Carcinoma
Abstract
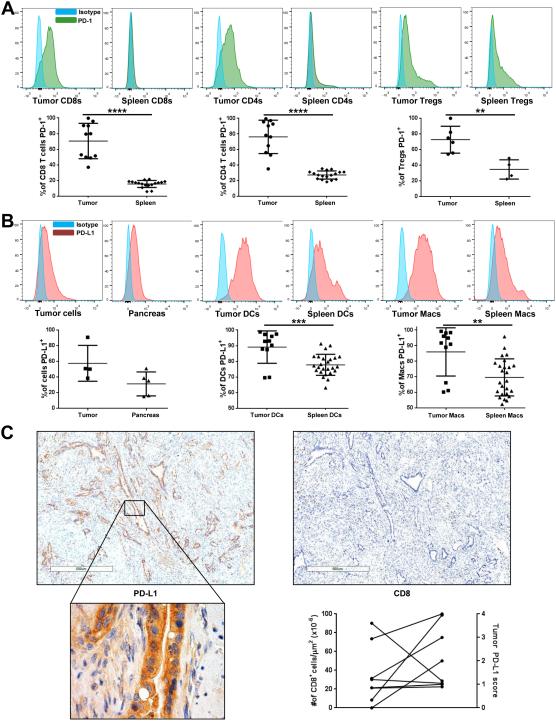
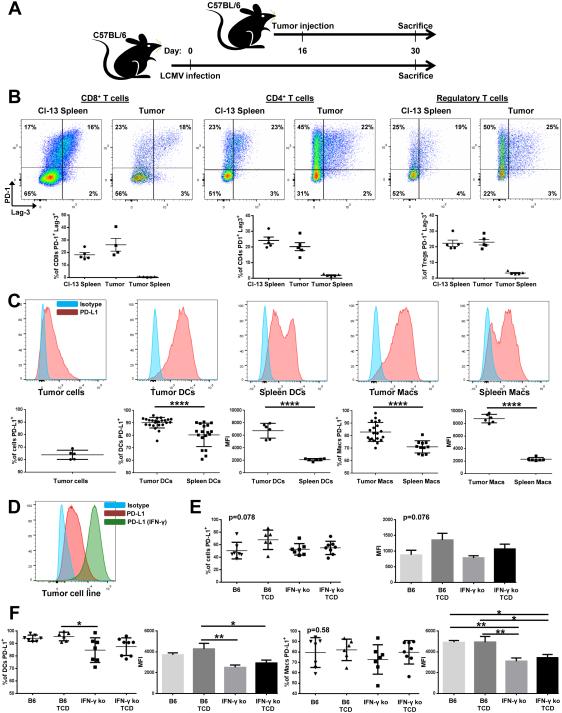
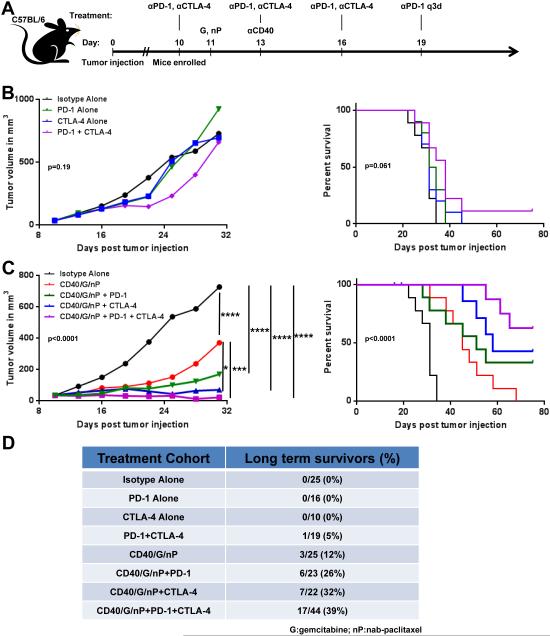
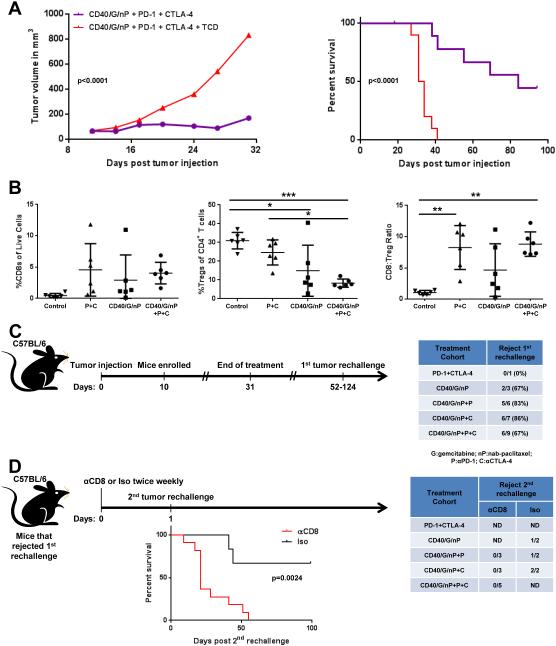
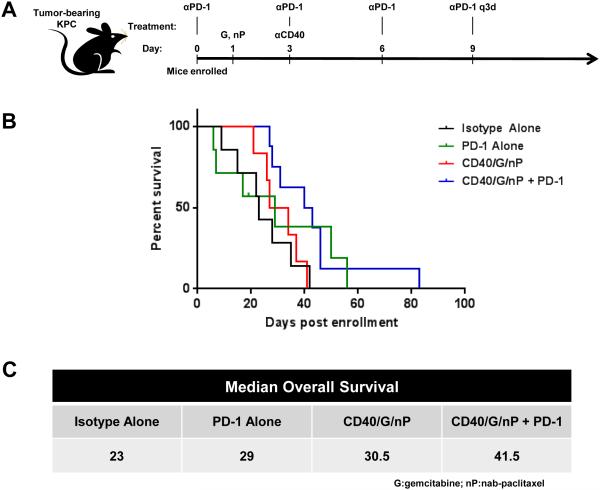
Disabling the function of immune checkpoint molecules can unlock T-cell immunity against cancer, yet despite remarkable clinical success with monoclonal antibodies (mAb) that block PD-1 or CTLA-4, resistance remains common and essentially unexplained. To date, pancreatic carcinoma is fully refractory to these antibodies. Here, using a genetically engineered mouse model of pancreatic ductal adenocarcinoma in which spontaneous immunity is minimal, we found that PD-L1 is prominent in the tumor microenvironment, a phenotype confirmed in patients; however, tumor PD-L1 was found to be independent of IFNγ in this model. Tumor T cells expressed PD-1 as prominently as T cells from chronically infected mice, but treatment with αPD-1 mAbs, with or without αCTLA-4 mAbs, failed in well-established tumors, recapitulating clinical results. Agonist αCD40 mAbs with chemotherapy induced T-cell immunity and reversed the complete resistance of pancreatic tumors to αPD-1 and αCTLA-4. The combination of αCD40/chemotherapy plus αPD-1 and/or αCTLA-4 induced regression of subcutaneous tumors, improved overall survival, and conferred curative protection from multiple tumor rechallenges, consistent with immune memory not otherwise achievable. Combinatorial treatment nearly doubled survival of mice with spontaneous pancreatic cancers, although no cures were observed. Our findings suggest that in pancreatic carcinoma, a nonimmunogenic tumor, baseline refractoriness to checkpoint inhibitors can be rescued by the priming of a T-cell response with αCD40/chemotherapy.
©2015 American Association for Cancer Research.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–21. - PubMed
-
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25. - PubMed
-
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity's roles in cancer suppression and promotion. Science. 2011;331:1565–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
