

Estimation of daily interfractional larynx residual setup error after isocentric alignment for head and neck radiotherapy: quality assurance implications for target volume and organs-at-risk margination using daily CT on- rails imaging
- PMID: 25679151
- PMCID: PMC5016194
- DOI: 10.1120/jacmp.v16i1.5108
Estimation of daily interfractional larynx residual setup error after isocentric alignment for head and neck radiotherapy: quality assurance implications for target volume and organs-at-risk margination using daily CT on- rails imaging
Abstract
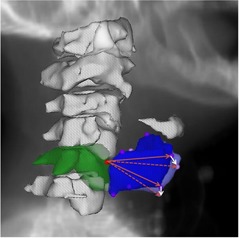
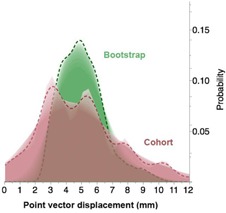
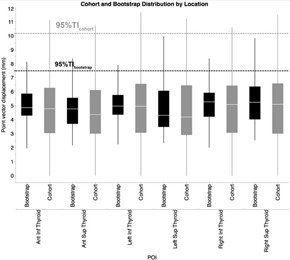
Larynx may alternatively serve as a target or organs at risk (OAR) in head and neck cancer (HNC) image-guided radiotherapy (IGRT). The objective of this study was to estimate IGRT parameters required for larynx positional error independent of isocentric alignment and suggest population-based compensatory margins. Ten HNC patients receiving radiotherapy (RT) with daily CT on-rails imaging were assessed. Seven landmark points were placed on each daily scan. Taking the most superior-anterior point of the C5 vertebra as a reference isocenter for each scan, residual displacement vectors to the other six points were calculated postisocentric alignment. Subsequently, using the first scan as a reference, the magnitude of vector differences for all six points for all scans over the course of treatment was calculated. Residual systematic and random error and the necessary compensatory CTV-to-PTV and OAR-to-PRV margins were calculated, using both observational cohort data and a bootstrap-resampled population estimator. The grand mean displacements for all anatomical points was 5.07 mm, with mean systematic error of 1.1 mm and mean random setup error of 2.63 mm, while bootstrapped POIs grand mean displacement was 5.09 mm, with mean systematic error of 1.23 mm and mean random setup error of 2.61 mm. Required margin for CTV-PTV expansion was 4.6 mm for all cohort points, while the bootstrap estimator of the equivalent margin was 4.9 mm. The calculated OAR-to-PRV expansion for the observed residual setup error was 2.7 mm and bootstrap estimated expansion of 2.9 mm. We conclude that the interfractional larynx setup error is a significant source of RT setup/delivery error in HNC, both when the larynx is considered as a CTV or OAR. We estimate the need for a uniform expansion of 5 mm to compensate for setup error if the larynx is a target, or 3 mm if the larynx is an OAR, when using a nonlaryngeal bony isocenter.
Figures
References
-
- van Herk M, Remeijer P, Lebesque JV. Inclusion of geometric uncertainties in treatment plan evaluation. Int J Radiat Oncol Biol Phys. 2002;52(5):1407–22. - PubMed
-
- Miszczyk L, Tarnawski R, Skladowski K. The impact of delivered dose errors on local control of irradiated advanced laryngeal cancer. Neoplasma. 2000;47(2):133–36. - PubMed
-
- Prescribing, recording, and reporting photon beam therapy (supplement to ICRU Report 50). ICRU Report 62. Bethesda, MD: ICRU; 1999.
-
- Prescribing, recording, and reporting photon‐beam intensity‐modulated radiation therapy (IMRT): contents. J ICRU. 2010;10(1). - PubMed
-
- Purdy JA. Current ICRU definitions of volumes: limitations and future directions. Sem Radiat Oncol. 2004;14(1):27–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
