

Interocular retinal nerve fiber layer thickness difference in normal adults
- PMID: 25679786
- PMCID: PMC4332477
- DOI: 10.1371/journal.pone.0116313
Interocular retinal nerve fiber layer thickness difference in normal adults
Abstract
Purpose: To determine the interocular retinal nerve fiber layer (RNFL) thickness difference of normal subjects.
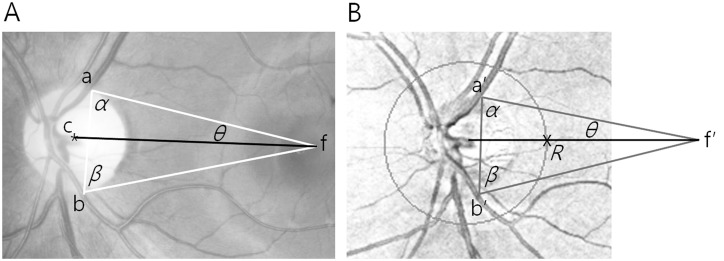
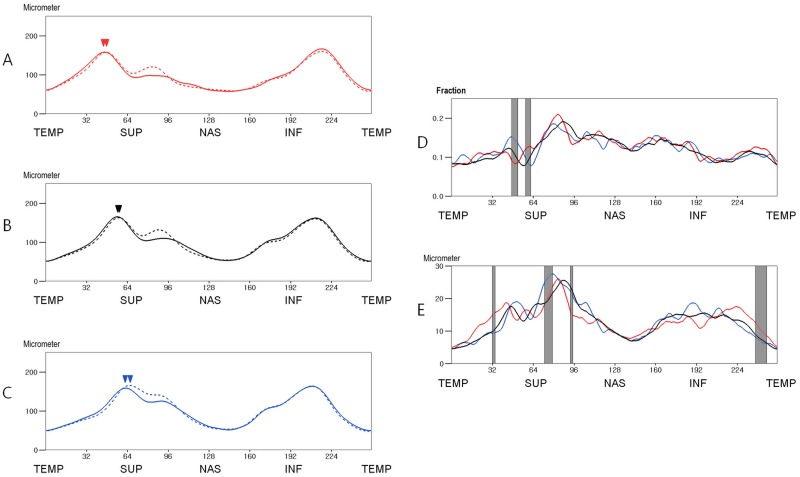
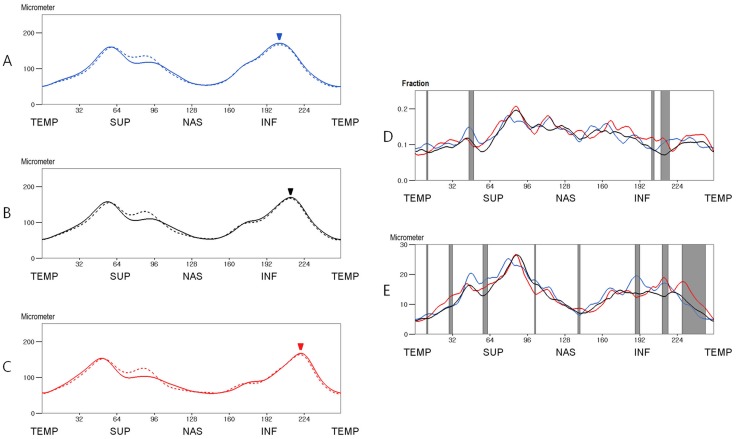
Methods: Both eyes of 230 normal adults received peripapillary RNFL thickness measurements using OCT. The effect of ocular cyclotorsion on the RNFL thickness profile was mathematically corrected. The fractional and absolute interocular RNFL thickness differences at 256 points of peripapillary area were calculated. We divided the subjects into 3 groups according to the locations of superior and inferior peak thickness, respectively, and compared the interocular RNFL thickness differences between the subgroups.
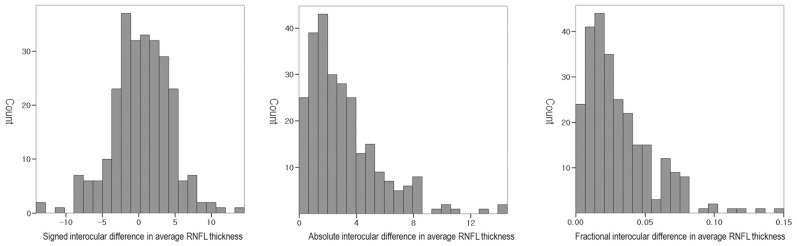
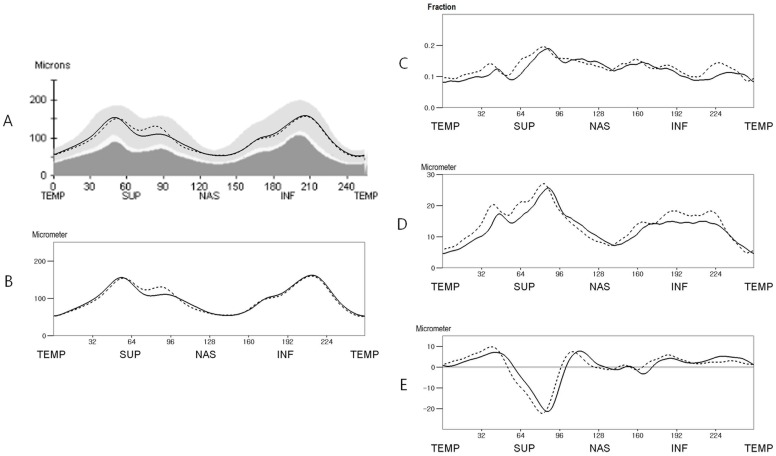
Results: The fractional interocular RNFL thickness difference exhibited smaller regional variations than the absolute interocular difference. The means of fractional interocular differences were 0.100 ± 0.077 in the temporal half area and 0.146 ± 0.105 in the nasal half area, and the tolerance limits for the 95th and 99 th distributions were about 0.246 and 0.344 in the temporal half area and 0.293 and 0.408 in the nasal half area, respectively. The fractional interocular differences of subgroups classified by the locations of superior and inferior peak RNFL thickness showed difference at smaller areas than the absolute interocular differences (19 and 8 points versus 49 and 23 points, respectively).
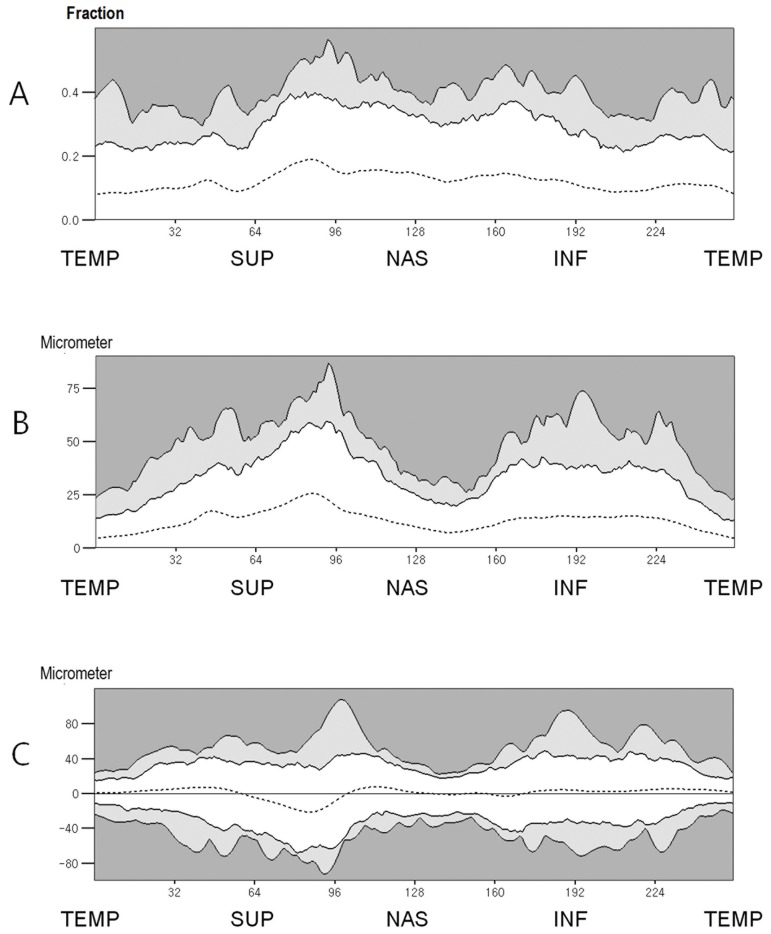
Conclusion: Glaucoma can be strongly suspected, if interocular fractional RNFL thickness difference is over 25% at 5 consecutive points or over 35% at 3 consecutive points in the temporal half area. The fractional interocular comparison is a better diagnostic approach because the fractional interocular RNFL thickness difference is less influenced by the locations of peak RNFL thickness.
Conflict of interest statement
Figures
References
-
- Budenz DL, Michael A, Chang RT, McSoley J, Katz J. Sensitivity and specificity of the stratus OCT for perimetric glaucoma. Ophthalmology. 2005;112:3–9. - PubMed
-
- Hougaard JL, Heiji A, Bengtsson B. Glaucoma detection using different stratus optical coherence tomography protocols. Acta Ophthalmol Scand. 2007;85:251–256. - PubMed
-
- Kanamori A, Nagai-Kusuhara A, Escano MF, Maeda H, Nakamura M, et al. Comparison of confocal scanning laser ophthalmoscopy, scanning laser polarimetry and optical coherence tomography to discriminate ocular hypertension and glaucoma at an early stage. Graefes Arch Clin Exp Ophthalmol. 2006;244:58–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
