

Development and validation of an internationally-standardized, high-resolution capillary gel-based electrophoresis PCR-ribotyping protocol for Clostridium difficile
- PMID: 25679978
- PMCID: PMC4332677
- DOI: 10.1371/journal.pone.0118150
Development and validation of an internationally-standardized, high-resolution capillary gel-based electrophoresis PCR-ribotyping protocol for Clostridium difficile
Abstract
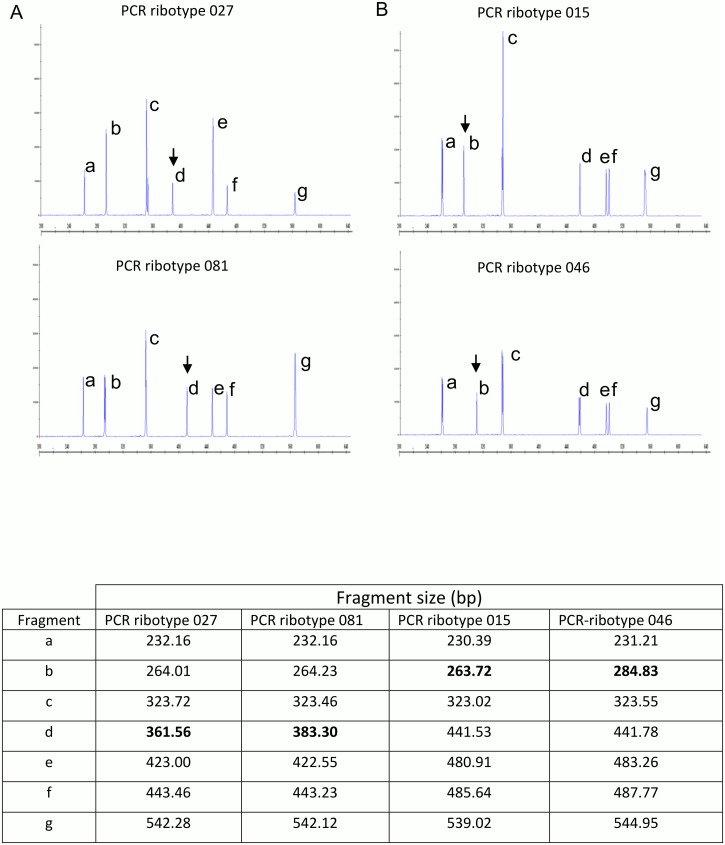
PCR-ribotyping has been adopted in many laboratories as the method of choice for C. difficile typing and surveillance. However, issues with the conventional agarose gel-based technique, including inter-laboratory variation and interpretation of banding patterns have impeded progress. The method has recently been adapted to incorporate high-resolution capillary gel-based electrophoresis (CE-ribotyping), so improving discrimination, accuracy and reproducibility. However, reports to date have all represented single-centre studies and inter-laboratory variability has not been formally measured or assessed. Here, we achieved in a multi-centre setting a high level of reproducibility, accuracy and portability associated with a consensus CE-ribotyping protocol. Local databases were built at four participating laboratories using a distributed set of 70 known PCR-ribotypes. A panel of 50 isolates and 60 electronic profiles (blinded and randomized) were distributed to each testing centre for PCR-ribotype identification based on local databases generated using the standard set of 70 PCR-ribotypes, and the performance of the consensus protocol assessed. A maximum standard deviation of only ±3.8bp was recorded in individual fragment sizes, and PCR-ribotypes from 98.2% of anonymised strains were successfully discriminated across four ribotyping centres spanning Europe and North America (98.8% after analysing discrepancies). Consensus CE-ribotyping increases comparability of typing data between centres and thereby facilitates the rapid and accurate transfer of standardized typing data to support future national and international C. difficile surveillance programs.
Conflict of interest statement
Figures

References
-
- Wiegand PN, Nathwani D, Wilcox MH, Stephens J, Shelbaya A, et al. Clinical and economic burden of Clostridium difficile infection in Europe: a systematic review of healthcare-facility-acquired infection. J Hosp Infect. 2012;77: 1–14. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
