

Effects of exercise training on neurovascular control and skeletal myopathy in systolic heart failure
- PMID: 25681428
- PMCID: PMC4398863
- DOI: 10.1152/ajpheart.00830.2014
Effects of exercise training on neurovascular control and skeletal myopathy in systolic heart failure
Abstract
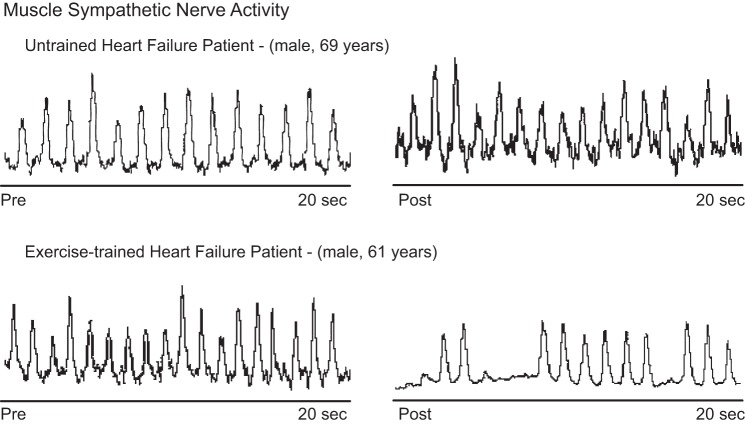
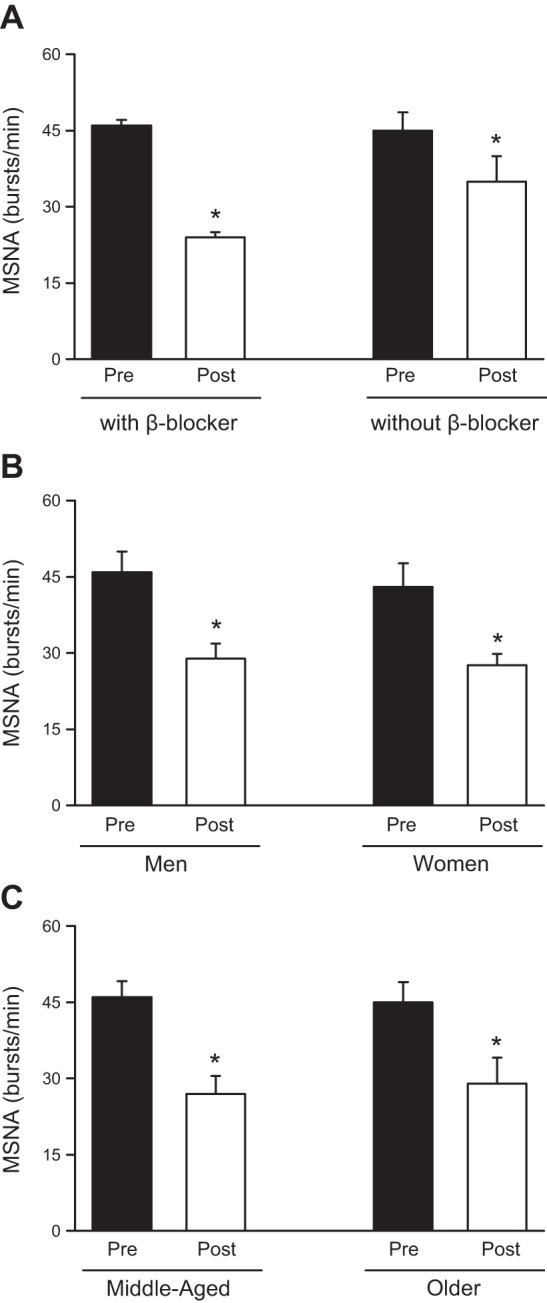
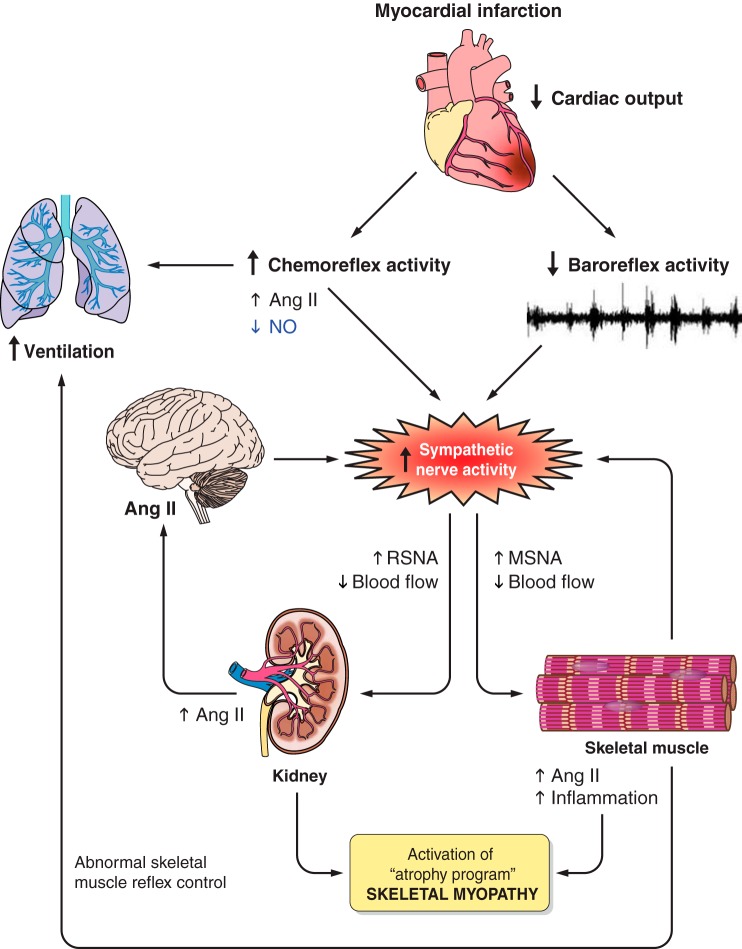
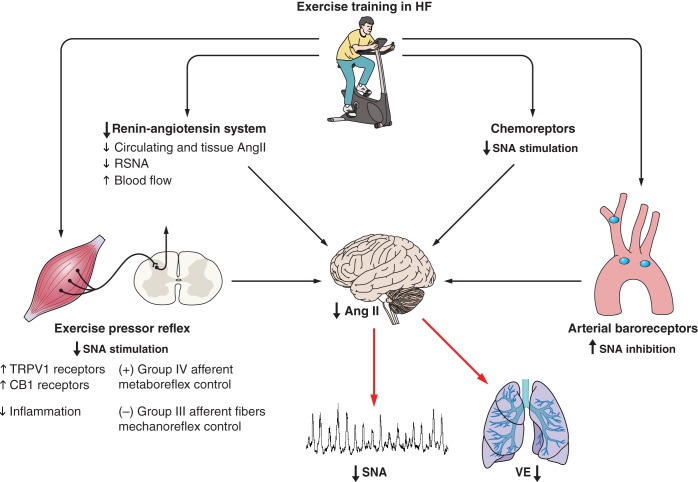
Neurohormonal excitation and dyspnea are the hallmarks of heart failure (HF) and have long been associated with poor prognosis in HF patients. Sympathetic nerve activity (SNA) and ventilatory equivalent of carbon dioxide (VE/VO2) are elevated in moderate HF patients and increased even further in severe HF patients. The increase in SNA in HF patients is present regardless of age, sex, and etiology of systolic dysfunction. Neurohormonal activation is the major mediator of the peripheral vasoconstriction characteristic of HF patients. In addition, reduction in peripheral blood flow increases muscle inflammation, oxidative stress, and protein degradation, which is the essence of the skeletal myopathy and exercise intolerance in HF. Here we discuss the beneficial effects of exercise training on resting SNA in patients with systolic HF and its central and peripheral mechanisms of control. Furthermore, we discuss the exercise-mediated improvement in peripheral vasoconstriction in patients with HF. We will also focus on the effects of exercise training on ventilatory responses. Finally, we review the effects of exercise training on features of the skeletal myopathy in HF. In summary, exercise training plays an important role in HF, working synergistically with pharmacological therapies to ameliorate these abnormalities in clinical practice.
Keywords: exercise training; heart failure; skeletal myopathy; sympathetic nerve activity; vasoconstriction.
Copyright © 2015 the American Physiological Society.
Figures
References
-
- Adamopoulos S, Coats AJ, Brunotte F, Arnolda L, Meyer T, Thompson CH, Dunn JF, Stratton J, Kemp GJ, Radda GK. Physical training improves skeletal muscle metabolism in patients with chronic heart failure. J Am Coll Cardiol 21: 1101–1106, 1993. - PubMed
-
- Alves MJ, Rondon MU, Santos AC, Dias RG, Barretto AC, Krieger EM, Middlekauff HR, Negrão CE. Sympathetic nerve activity restrains reflex vasodilatation in heart failure. Clin Auton Res 17: 364–369, 2007. - PubMed
-
- Anker SD, Swan JW, Volterrani M, Chua TP, Clark AL, Poole-Wilson PA, Coats AJ. The influence of muscle mass, strength, fatigability and blood flow on exercise capacity in cachectic and non-cachectic patients with chronic heart failure. Eur Heart J 18: 259–269, 1997. - PubMed
-
- Antunes-Correa LM, Kanamura BY, Melo RC, Nobre TS, Ueno LM, Franco FG, Roveda F, Braga AM, Rondon MU, Brum PC, Barretto AC, Middlekauff HR, Negrao CE. Exercise training improves neurovascular control and functional capacity in heart failure patients regardless of age. Eur J Prev Cardiol 19: 822–829, 2012. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous