

Gender differences in pre-event health status of young patients with acute myocardial infarction: A VIRGO study analysis
- PMID: 25681487
- PMCID: PMC4658311
- DOI: 10.1177/2048872615568967
Gender differences in pre-event health status of young patients with acute myocardial infarction: A VIRGO study analysis
Abstract
Aims: We assessed gender differences in pre-event health status (symptoms, functioning, quality of life) in young patients with acute myocardial infarction and whether or not this association persists following sequential adjustment for important covariates. We also evaluated the interaction between gender and prior coronary artery disease, given that aggressive symptom control is a cornerstone of care in those with known coronary disease.
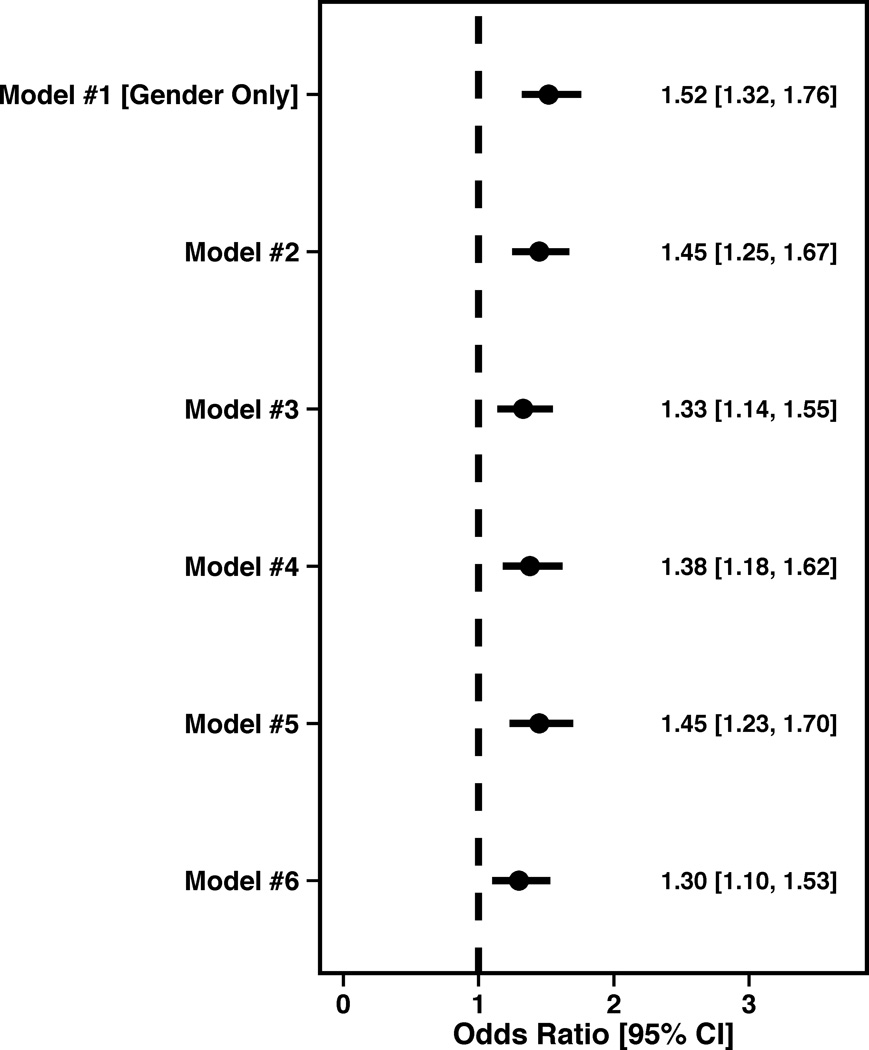
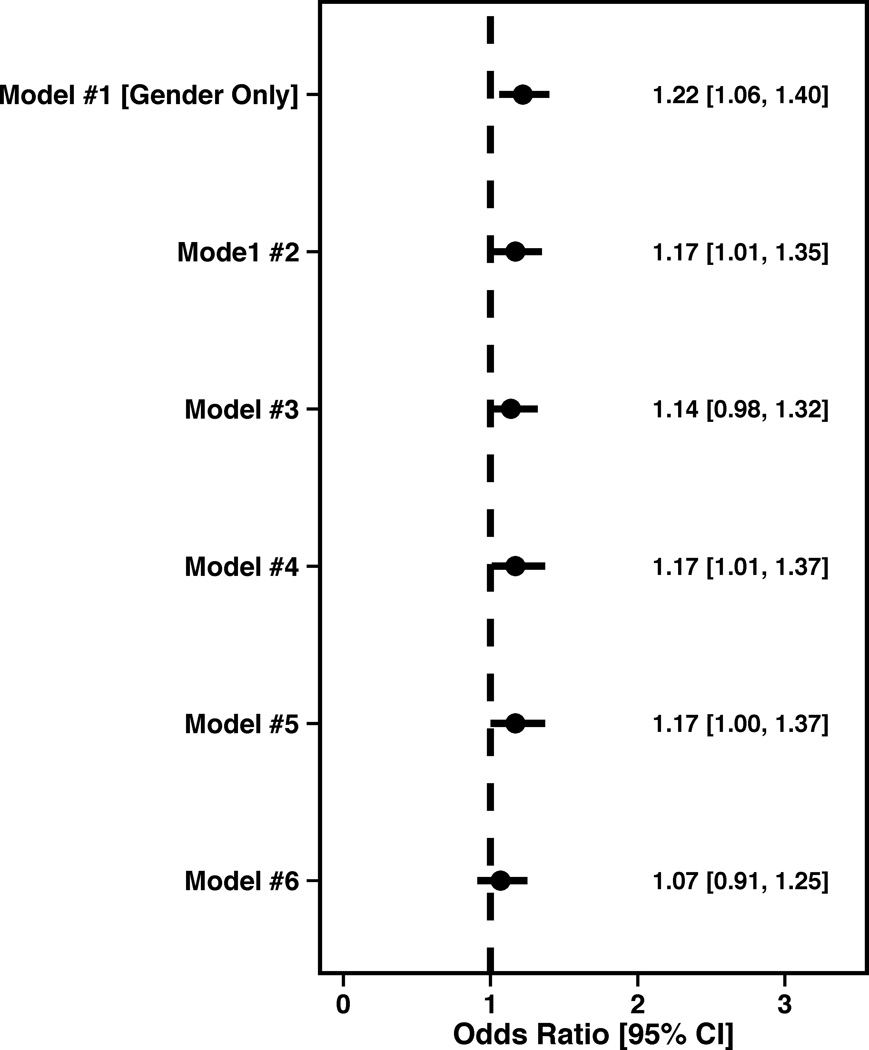
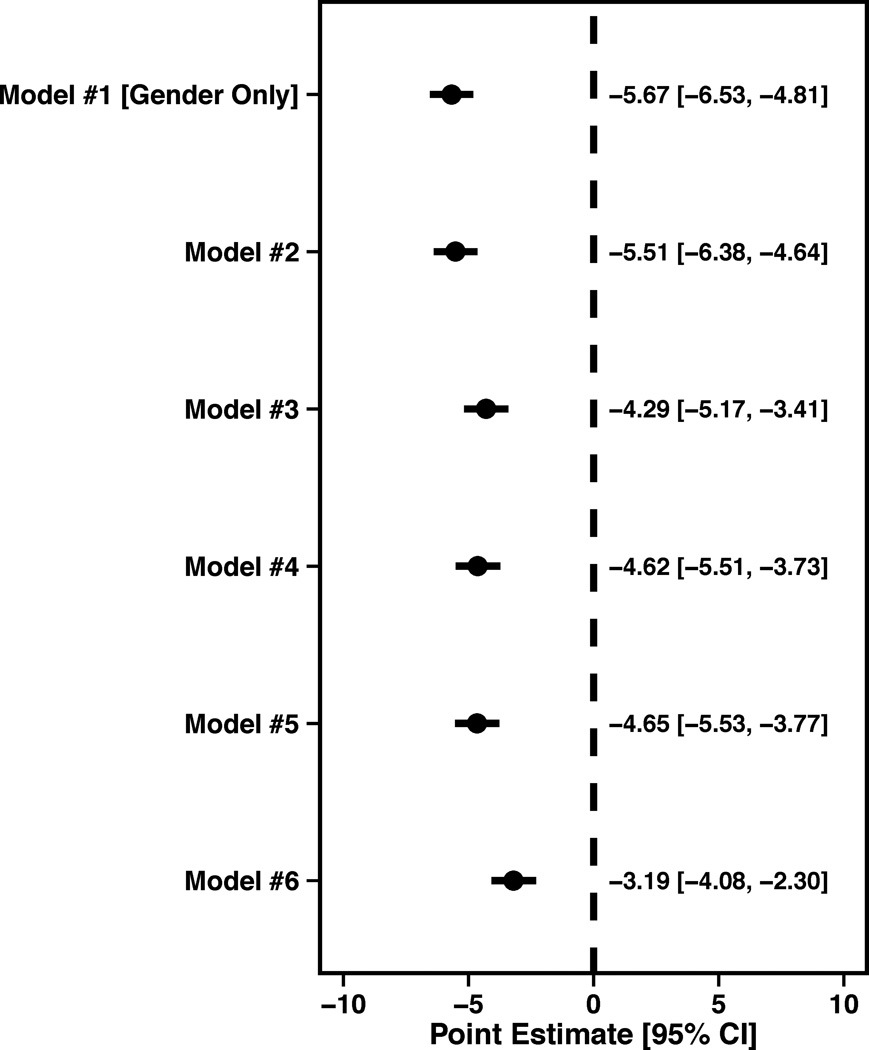
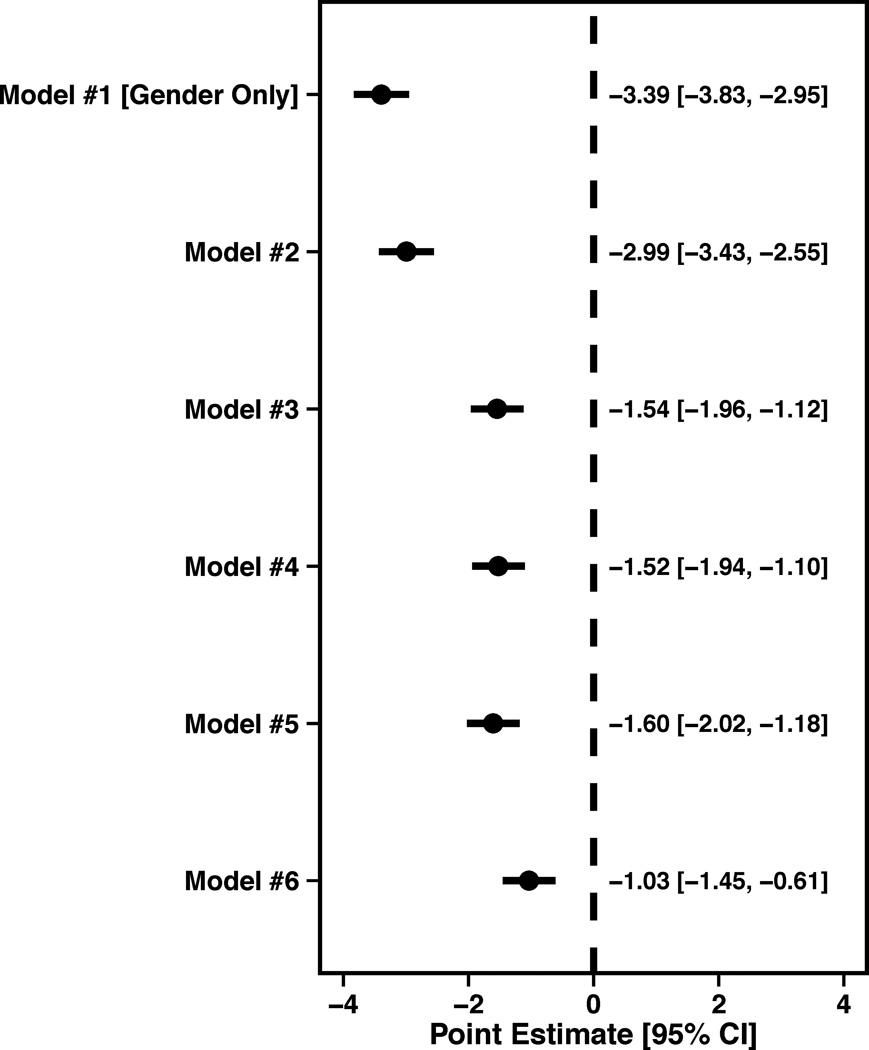
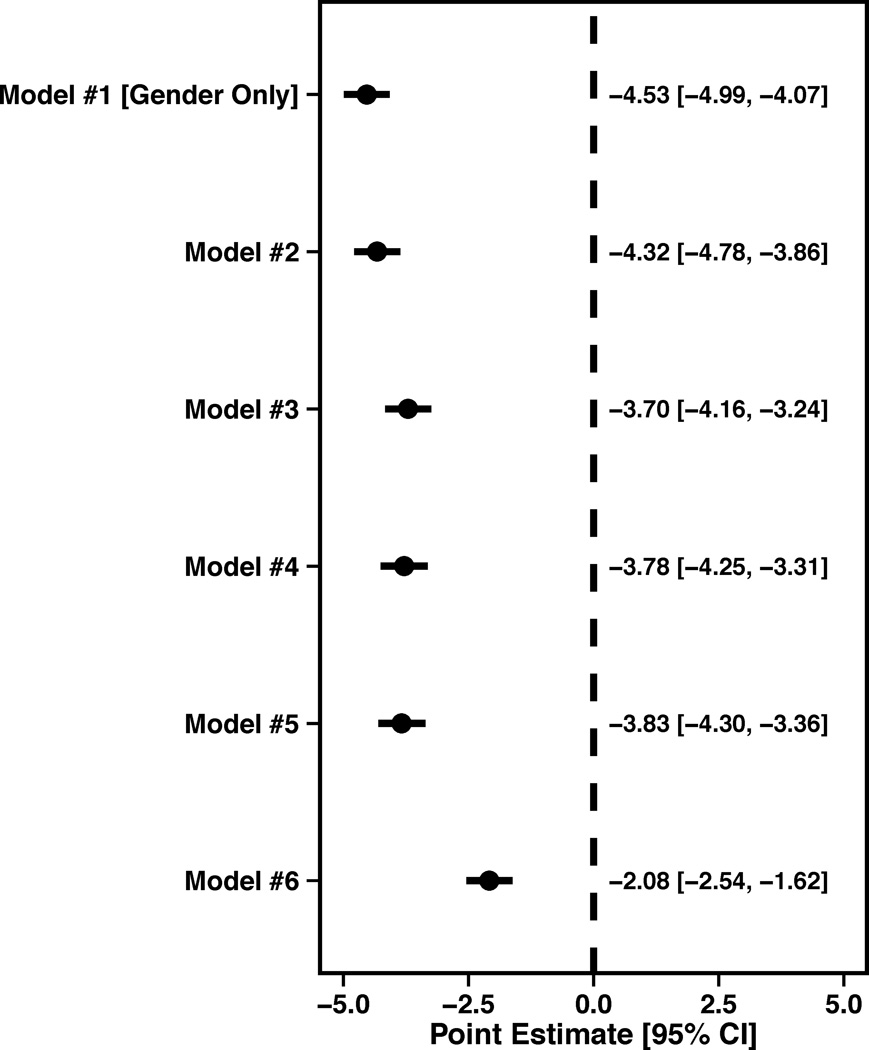
Methods and results: A total of 3501 acute myocardial infarction patients (2349 women) aged 18-55 years were enrolled from 103 US/24 Spanish hospitals (2008-2012). Clinical/health status information was obtained by medical record abstraction and patient interviews. Pre-event health status was measured by generic (Short Form-12, EuroQoL) and disease-specific (Seattle Angina Questionnaire) measures. T-test/chi-square and multivariable linear/logistic regression analysis was utilized, sequentially adjusting for covariates. Women had more co-morbidities and significantly lower generic mean health scores than men (Short Form-12 physical health = 43 ± 12 vs. 46 ± 11 and mental health = 44 ± 13 vs. 48 ± 11); EuroQoL utility index = 0.7 ± 0.2 vs. 0.8 ± 0.2 and visual analog scale = 63 ± 22 vs. 67 ± 20, P < 0.0001 for all. Their disease-specific health status was also worse, with more angina (Seattle Angina Questionnaire angina frequency = 83 ± 22 vs. 87 ± 18), worse physical function (physical limitation = 78 ± 27 vs. 87 ± 21) and poorer quality of life (55 ± 25 vs. 60 ± 22, P<0.0001 for all). In multivariable analysis, the association between female gender and worse generic physical/mental health persisted, as well as worse disease-specific physical limitation and quality of life. The interaction between gender and prior coronary artery disease was not significant in any of the health status outcomes.
Conclusion: Young women have worse pre-event health status as compared with men, regardless of their coronary artery disease history. While future studies of gender differences should adjust for baseline health status, an opportunity may exist to better address the pre-event health status of women at risk for acute myocardial infarction.
Keywords: Health status; acute myocardial infarction; quality of life; women.
© The European Society of Cardiology 2015.
Conflict of interest statement
Figures
References
-
- Vaccarino V, Parsons L, Every NR, et al. Sex-based differences in early mortality after myocardial infarction. National registry of myocardial infarction 2 participants. N Engl J Med. 1999;341(4):217–225. - PubMed
-
- Vaccarino V, Horwitz RI, Meehan TP, et al. Sex differences in mortality after myocardial infarction: Evidence for a sex-age interaction. Arch Intern Med. 1998;158(18):2054–2062. - PubMed
-
- Pedersen SS, Martens EJ, Denollet J, et al. Poor health-related quality of life is a predictor of early, but not late, cardiac events after percutaneous coronary intervention. Psychosomatics. 2007;48(4):331–337. - PubMed
-
- Spertus JA, Jones P, McDonell M, et al. Health status predicts long-term outcome in outpatients with coronary disease. Circulation. 2002;106(1):43–49. - PubMed
-
- Spertus JA. Evolving applications for patient-centered health status measures. Circulation. 2008;118(20):2103–2110. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
