

Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study
- PMID: 25682233
- PMCID: PMC4404207
- DOI: 10.1016/S2213-2600(15)00043-0
Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study
Abstract
Background: Sleep-disordered breathing is associated with major morbidity and mortality. However, its prevalence has mainly been selectively studied in populations at risk for sleep-disordered breathing or cardiovascular diseases. Taking into account improvements in recording techniques and new criteria used to define respiratory events, we aimed to assess the prevalence of sleep-disordered breathing and associated clinical features in a large population-based sample.
Methods: Between Sept 1, 2009, and June 30, 2013, we did a population-based study (HypnoLaus) in Lausanne, Switzerland. We invited a cohort of 3043 consecutive participants of the CoLaus/PsyCoLaus study to take part. Polysomnography data from 2121 people were included in the final analysis. 1024 (48%) participants were men, with a median age of 57 years (IQR 49-68, range 40-85) and mean body-mass index (BMI) of 25·6 kg/m(2) (SD 4·1). Participants underwent complete polysomnographic recordings at home and had extensive phenotyping for diabetes, hypertension, metabolic syndrome, and depression. The primary outcome was prevalence of sleep-disordered breathing, assessed by the apnoea-hypopnoea index.
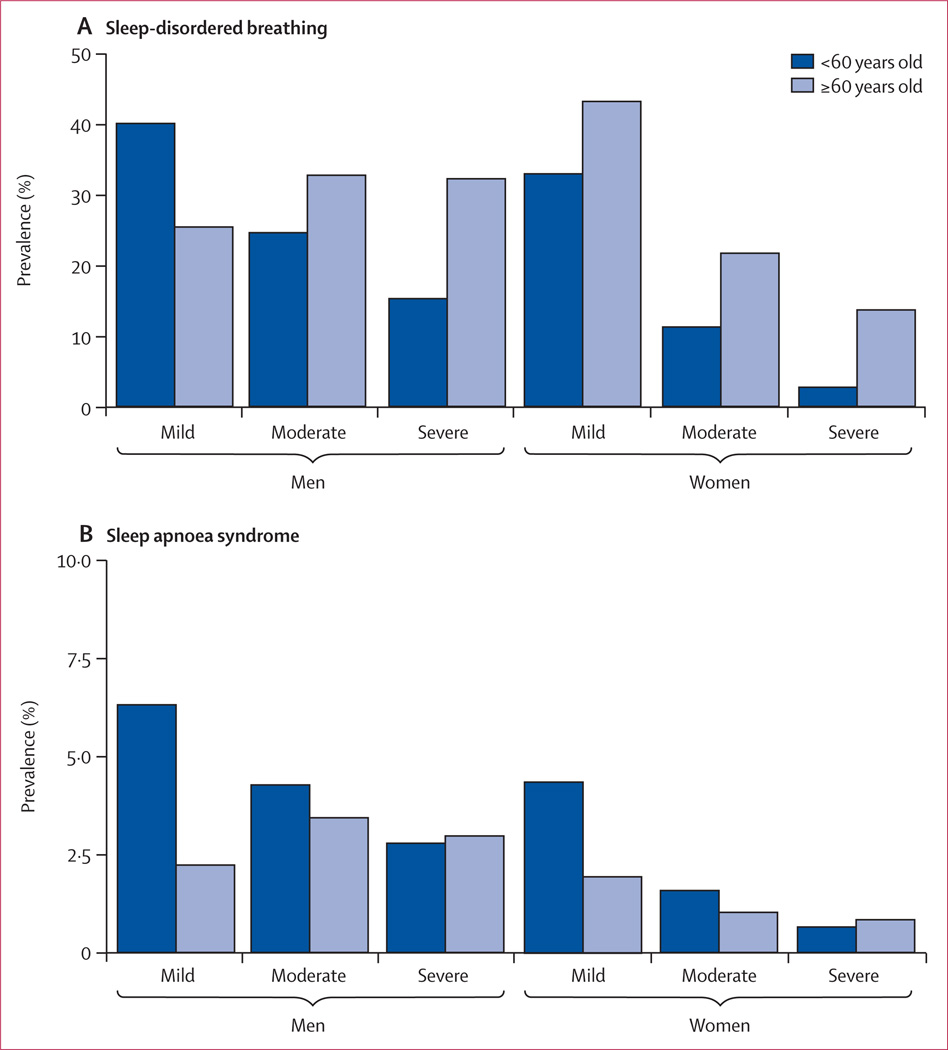
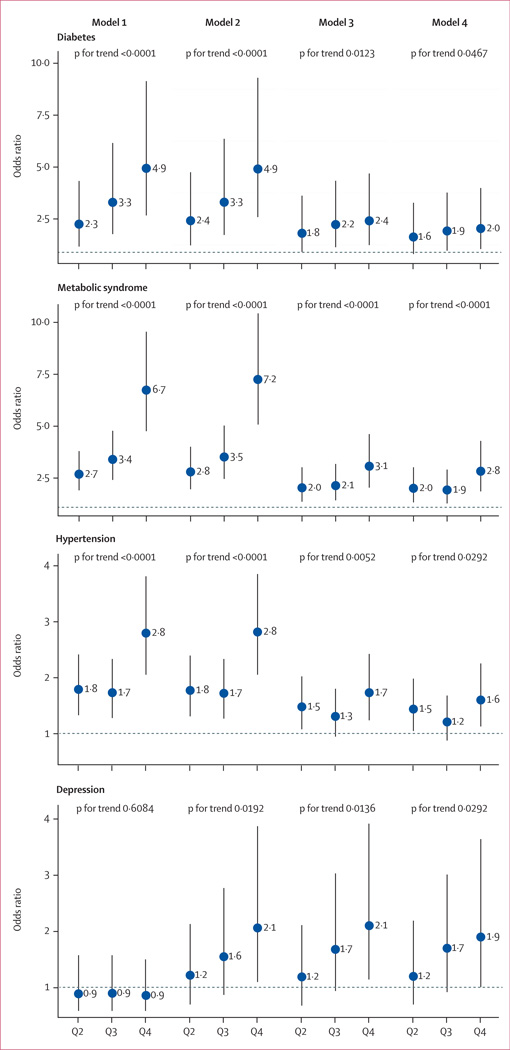
Findings: The median apnoea-hypopnoea index was 6·9 events per h (IQR 2·7-14·1) in women and 14·9 per h (7·2-27·1) in men. The prevalence of moderate-to-severe sleep-disordered breathing (≥15 events per h) was 23·4% (95% CI 20·9-26·0) in women and 49·7% (46·6-52·8) in men. After multivariable adjustment, the upper quartile for the apnoea-hypopnoea index (>20·6 events per h) was associated independently with the presence of hypertension (odds ratio 1·60, 95% CI 1·14-2·26; p=0·0292 for trend across severity quartiles), diabetes (2·00, 1·05-3·99; p=0·0467), metabolic syndrome (2·80, 1·86-4·29; p<0·0001), and depression (1·92, 1·01-3·64; p=0·0292).
Interpretation: The high prevalence of sleep-disordered breathing recorded in our population-based sample might be attributable to the increased sensitivity of current recording techniques and scoring criteria. These results suggest that sleep-disordered breathing is highly prevalent, with important public health outcomes, and that the definition of the disorder should be revised.
Funding: Faculty of Biology and Medicine of Lausanne, Lausanne University Hospital, Swiss National Science Foundation, Leenaards Foundation, GlaxoSmithKline, Ligue Pulmonaire Vaudoise.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Prevalence and classification of sleep-disordered breathing.Lancet Respir Med. 2015 Apr;3(4):263-4. doi: 10.1016/S2213-2600(15)00054-5. Epub 2015 Feb 20. Lancet Respir Med. 2015. PMID: 25704990 No abstract available.
-
Are the ICSD-3 criteria for sleep apnoea syndrome too inclusive?Lancet Respir Med. 2016 May;4(5):e19-20. doi: 10.1016/S2213-2600(16)00109-0. Lancet Respir Med. 2016. PMID: 27304561 No abstract available.
References
-
- Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–1384. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–2041. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
